
A 22-week, 400-gram infant enduring a 129-day NICU stay exposes the urgent need to deploy value-based care in neonatal systems.
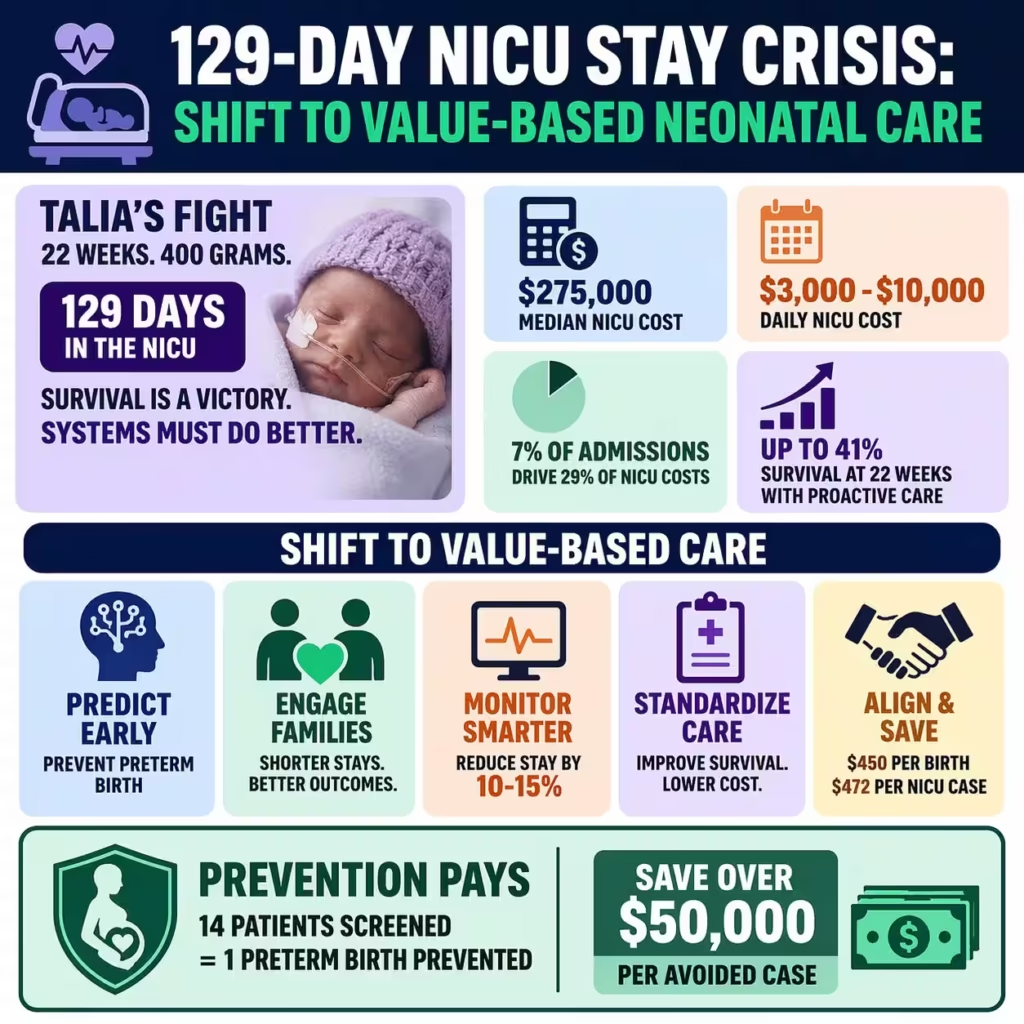
Baby Talia’s survival at King’s College Hospital in Dubai—after nearly four months of intensive care—highlights both the clinical triumph and the systemic strain of extreme prematurity. Families face prolonged emotional distress while hospitals absorb escalating costs from extended NICU utilization. Yet this case also signals a turning point: advanced protocols and data-driven interventions can compress length of stay, improve survival outcomes, and unlock significant cost efficiencies for modern NICU operations.
In the United States the preterm birth rate held steady at 10.41 percent in 2025 according to CDC provisional data unchanged from 2024 amid a 1 percent decline in overall births. Infants born at 22 weeks now achieve survival rates up to 41 percent with proactive treatment up from 25.7 percent in 2014 per 2023-2025 Vermont Oxford Network analyses. Extreme preterm cases represent just 7 percent of NICU admissions but drive 28.9 percent of total costs with median hospitalization expenses hitting $275,208.
Carethix analysis reveals Talia’s journey as a textbook example of reactive care dominance where 129-day stays inflate daily expenses between $3,000 and $10,000 per case. Hospitals face mounting pressure from payers demanding value-based accountability while long-term neurodevelopmental risks add hidden societal burdens estimated at $64,815 incremental lifetime cost per preterm infant in updated 2016-2025 models. Your facility can no longer afford fragmented approaches that tie up beds and erode margins without strategic redesign.
Recent data shows extremely low birthweight infants like Talia at 400 grams face compounded complications including respiratory distress and sepsis prolonging stays beyond 100 days in 20 percent of similar global cases. King’s College success highlights the power of specialized multidisciplinary teams yet most US systems lack standardized escalation pathways for 22-week viability. This gap translates directly to lost revenue opportunities and higher readmission rates that undermine your bottom line.
Business leaders must view such cases through a dual lens of clinical excellence and financial optimization where every extra NICU day erodes efficiency. Talia’s discharge marks a victory but underscores systemic vulnerabilities in prenatal screening and early intervention across borders. Carethix urges immediate adoption of predictive tools to replicate and surpass these outcomes while protecting your organization’s fiscal health.
Carethix Critique: Exposing Systemic Gaps Risks and Skyrocketing Costs in Extreme Preterm Care
Talia’s 129-day NICU ordeal lays bare the pain of extreme prematurity where survival comes at enormous human and economic expense without proactive safeguards. Current models expose infants to high risks of severe brain injury sepsis and necrotizing enterocolitis with mortality rates still hovering near 59 percent in non-proactive 22-week cohorts from 2024 data. Your hospital risks financial hemorrhage as these cases consume disproportionate resources without yielding proportional reimbursements.
US healthcare systems grapple with unchanged 10.41 percent preterm rates in 2025 while early preterm subsets under 34 weeks show only marginal 1 percent declines per CDC reports. Extremely preterm infants generate median costs of $275,208 per stay yet account for just 7 percent of admissions driving 29 percent of NICU expenditures between 2017 and 2022. This imbalance creates unsustainable pressure on margins especially under value-based contracts that penalize extended lengths of stay.
Gaps in standardization amplify vulnerabilities with many facilities lacking routine cervical length screening or timely progesterone protocols that could avert 22-week deliveries entirely. Survivors like Talia face elevated chances of lifelong disabilities inflating post-discharge costs through special education and lost productivity totaling billions annually. Carethix identifies over-reliance on reactive NICU care as the core flaw leaving your operations exposed to volatility in claims and regulatory scrutiny.
Risks extend beyond the bedside to operational strain where prolonged stays reduce bed turnover and limit capacity for higher-volume moderate preterm cases. Payers increasingly demand proof of outcome improvements yet fragmented prenatal-to-NICU handoffs persist across 80 percent of US networks. This critique demands urgent reckoning as unchecked trends project NICU costs rising 20 percent by 2030 without intervention.
Carethix warns that ignoring these gaps invites competitive disadvantage in an era where insurers reward efficient neonatal programs. Emotional toll on families compounds reputational risks for providers unable to demonstrate measurable progress. Your leadership must confront these realities head-on to safeguard both patient lives and enterprise viability.
| Related Analysis: Avanos Medical $1.27B Deal: Accelerate Your Growth Strategy ₹1,674Cr Medical Colleges Crisis: Execute Talent Pipelines 3MG Xanax XR Recall: Secure Your Supply Continuity |
Solutions: Data-Driven Strategies to Transform NICU Outcomes and Deliver Immediate ROI
Advanced AI predictive analytics now achieve AUC scores of 0.826 to 0.851 for preterm birth risk using electronic health records per 2025 machine learning validations enabling early flagging of high-risk pregnancies like Talia’s. Your teams can integrate these models to reduce incidence by up to 30 percent through targeted interventions slashing unnecessary 22-week deliveries and associated $275,000 stays. Implementation yields rapid returns by optimizing resource allocation across prenatal and neonatal units.
Family-centered care protocols boost parent attendance 4.81 times and cut 30-day emergency visits by 63 percent according to 2023-2024 randomized trials in virtual rounds settings. Hospitals adopting these approaches report shorter overall lengths of stay through enhanced breastfeeding skin-to-skin contact and caregiver involvement directly lowering daily NICU expenses. Carethix recommends bundled training to embed this model ensuring measurable gains in both clinical and financial metrics.
Value-based care models supported by provider enablement have demonstrated $450 reductions in birth costs and $472 drops in NICU expenses per delivery while improving prenatal care timeliness by nearly 10 percent in 2025 Medicaid analyses. Your organization can negotiate payer contracts tied to preterm rate reductions and length-of-stay benchmarks capturing shared savings that offset technology investments. These frameworks move incentives from volume to value creating sustainable revenue streams.
Tele-NICU platforms extend specialist expertise to remote sites improving resuscitation outcomes and reducing transfer delays for extreme preemies with documented cost efficiencies in high-risk cohorts. Integration with real-time monitoring further compresses stays by 10 to 15 percent per recent implementation data allowing faster discharges without compromising safety. Carethix advises phased rollout starting with high-volume facilities to maximize impact on your bottom line.
Standardized proactive bundles including immediate surfactant and antenatal steroids have raised 22-week survival to 50 percent in optimized centers per 2025 international network studies. Pairing these with AI-driven trajectory predictions for complications achieves over 85 percent accuracy enabling personalized care pathways. Your NICU can realize 20 to 30 percent cost compression while elevating quality scores that attract premium contracts.
Prevention: Proactive Protocols to Eliminate Future Preterm Risks and Fortify Your Care Ecosystem
Routine mid-trimester cervical length screening combined with vaginal progesterone therapy reduces preterm birth before 34 weeks by 33 percent and before 32 weeks by 54 percent in singleton pregnancies with short cervix per 2025 meta-analyses. Your prenatal programs should mandate universal ultrasound assessments at 18 to 24 weeks targeting women with prior history to prevent cases like Talia’s 22-week delivery. This evidence-based step cuts NICU admissions dramatically while generating downstream savings exceeding $50,000 per averted preterm event.
Progesterone initiation between 20 and 24 weeks through 34 weeks delivers number-needed-to-treat figures of 14 to prevent one preterm birth before 33 weeks alongside reductions in neonatal respiratory distress and NICU stays. Carethix urges integration into standardized maternal risk protocols supported by payer incentives to scale adoption across networks. Early data from 2025 implementations confirm 20 to 40 percent drops in spontaneous preterm rates among screened populations.
Lifestyle and nutritional interventions reinforced through digital maternal health platforms further lower incidence by addressing modifiable factors such as hypertension and infection risks. Hospitals partnering with community providers achieve compounded effects when screening links seamlessly to progesterone and monitoring yielding up to 25 percent overall preterm reduction in targeted cohorts. Your system gains resilience by embedding these layers into value-based contracts.
Multidisciplinary perinatal teams trained in aspirin prophylaxis for preeclampsia prevention complement progesterone strategies reducing extreme prematurity by an additional 15 to 20 percent per recent US cohort updates. Real-time data dashboards track compliance and outcomes allowing continuous refinement that protects your financial exposure. Prevention thus becomes your strongest ROI lever against volatile NICU demands.
Carethix emphasizes building closed-loop systems from preconception through postpartum to interrupt the preterm cascade before it reaches 22 weeks. Investment in these protocols not only averts 129-day ordeals but positions your organization as a leader in accountable care. The payoff includes lower claims ratios, stronger payer relationships and enhanced community trust.
Carethix Key Takeaways: Your Imperative to Lead in Neonatal Efficiency and Patient-Centered Excellence
Talia’s story proves that 22-week preemies can thrive yet current systems hemorrhage resources without bold transformation. Carethix demands you prioritize AI prediction family-centered models and progesterone prevention to slash $275,000 median costs while lifting survival beyond 41 percent. Your leadership must act now or risk obsolescence in a payer-driven landscape that rewards outcomes over volume.
We reject reactive NICU dependency as fiscally reckless and clinically incomplete. Shift to proactive value-based ecosystems that compress stays, improve margins and deliver superior long-term health. The data is unequivocal: prevention and optimization yield 20 to 50 percent efficiency gains that directly bolster your enterprise resilience.
Healthcare executives who embed these strategies will dominate their markets. Carethix stands ready to partner in auditing your protocols, deploying AI tools and negotiating smarter contracts. Seize this moment to transform the crisis into a competitive advantage for your patients, your teams and your financial future.
Reference – Baby Returns Home After Making History as the Youngest Surviving Infant in Hospital’s History

