
Repeated Implantation Failure (RIF), a 42.5% pregnancy crisis, demands that healthcare leaders build smarter IVF care and fertility strategies.
Deep Case Study: Immune Dysregulation Is Emerging as a Critical Barrier to Successful Embryo Implantation
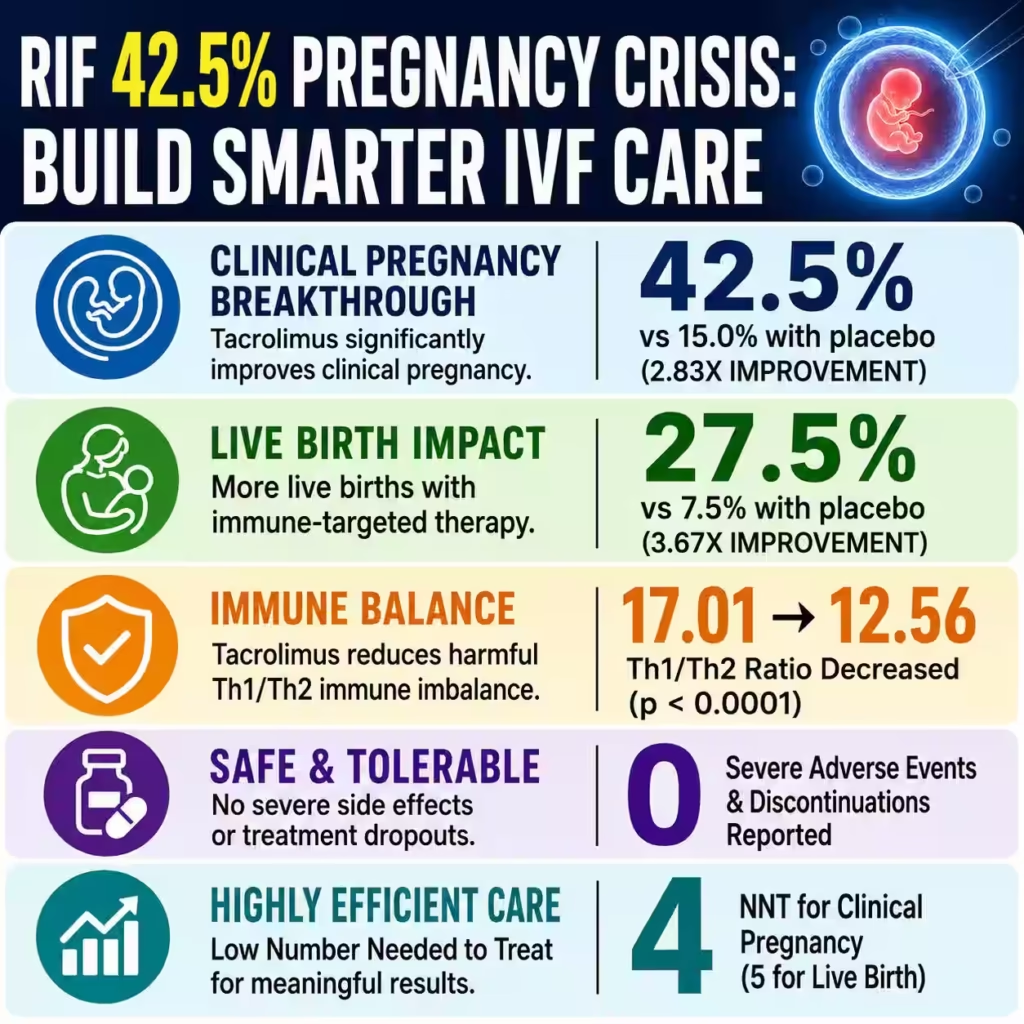
Repeated implantation failure (RIF) continues to challenge fertility medicine because even after transferring good-quality embryos, implantation does not occur in many patients. A randomized, double-blind, placebo-controlled trial conducted between April 2024 and May 2025 reported a 42.5% clinical pregnancy rate with tacrolimus compared with 15.0% with placebo, representing a 2.83-fold relative improvement, an absolute benefit of 27.5%, and a Number Needed to Treat (NNT) of just 4. These findings offer a meaningful direction for immune-guided fertility care while also emphasizing that immunosuppressive therapy should only be considered within carefully selected patient populations supported by laboratory evidence of immune dysregulation.
Repeated implantation failure affects a substantial proportion of couples undergoing assisted reproductive technology despite advances in embryo culture, embryo selection, and laboratory quality systems. Although definitions vary, many fertility programs define RIF as failure to achieve clinical pregnancy after multiple transfers of good-quality embryos. The economic burden is considerable because a single IVF cycle in many countries costs several thousand dollars while repeated unsuccessful cycles increase healthcare expenditure, emotional stress, and treatment discontinuation.
The randomized trial screened 153 women, identifying 91 patients with an elevated Th1/Th2 ratio of at least 10.3, a biomarker suggesting immune imbalance. Following exclusions, 80 patients underwent randomization in a 1:1 allocation, with 40 receiving tacrolimus and 40 receiving placebo. The study design incorporated randomization, double blinding, placebo control, predefined primary and secondary outcomes, and standardized treatment duration, representing one of the strongest clinical designs currently available for this specific subgroup of RIF patients.
The intervention consisted of administering tacrolimus for 16 consecutive days, beginning 2 days before embryo transfer and continuing until pregnancy testing. This timing targeted the implantation window, where maternal immune tolerance is essential for embryo acceptance. Unlike empirical immunotherapy, treatment was directed toward women with documented immune dysregulation rather than all patients experiencing implantation failure.
Clinical pregnancy occurred in 17 of 40 women (42.5%) receiving tacrolimus compared with only 6 of 40 women (15.0%) receiving placebo. The reported relative risk of 2.83 with a 95% confidence interval of 1.30–6.44 and p=0.0125 demonstrated statistical significance. An absolute improvement of 27.5 percentage points means approximately one additional successful pregnancy for every four treated patients, an outcome that carries important implications for reproductive medicine.
Live birth remains the most meaningful fertility outcome because successful implantation alone does not guarantee delivery of a healthy infant. The study demonstrated 11 live births among 40 patients (27.5%) receiving tacrolimus compared with 3 of 40 (7.5%) receiving placebo. The calculated relative risk of 3.67, 95% confidence interval of 1.21–11.63, p=0.0367, and an NNT of 5 suggest that immune-targeted therapy may influence clinically meaningful reproductive endpoints rather than merely biochemical pregnancy.
Immunological findings reinforce the biological validity of observed outcomes. The average Th1/Th2 ratio decreased from 17.01 ± 3.99 to 12.56 ± 2.78 following tacrolimus treatment with p<0.0001, while placebo recipients showed no statistically significant improvement. This reduction indicates that tacrolimus successfully moderated excessive Th1-mediated inflammatory activity, potentially improving endometrial receptivity during embryo implantation.
Safety remains a central concern whenever immunosuppressive medications are introduced into fertility treatment. Importantly, investigators reported no severe adverse events, no treatment discontinuations, and acceptable short-term tolerability during the study period. Although encouraging, these findings should not be interpreted as evidence of universal safety because the study involved only 80 randomized participants, and larger multicenter investigations are still necessary to better characterize maternal, fetal, and neonatal outcomes.
Globally, infertility affects approximately 1 in 6 adults during their lifetime according to recent international estimates, highlighting the scale of reproductive healthcare demand. Assisted reproductive technology continues to expand, with hundreds of thousands of IVF cycles performed annually across developed healthcare systems. Even modest improvements in implantation success can therefore translate into meaningful reductions in repeat procedures, cumulative treatment costs, emotional burden, and healthcare resource utilization.
The broader clinical significance extends beyond tacrolimus itself because the study reinforces precision reproductive medicine rather than universal treatment protocols. Instead of administering immunotherapy indiscriminately, clinicians may increasingly rely on immune biomarkers, cytokine profiles, and individualized patient stratification to guide therapy selection. This transition toward biomarker-driven fertility management aligns with broader healthcare trends emphasizing personalized medicine, evidence-based interventions, and measurable clinical outcomes.
From a healthcare consultancy perspective, the study represents an important operational lesson for fertility centers. Organizations that integrate immunological assessment, standardized laboratory pathways, multidisciplinary reproductive medicine teams, and outcome monitoring may improve both clinical effectiveness and resource allocation. The trial therefore contributes not only to therapeutic decision-making but also to the evolution of quality management frameworks within reproductive healthcare delivery.
Carethix Analysis: The Evidence Is Encouraging, but Immune-Targeted Fertility Care Still Faces Important Clinical Gaps
From Carethix’s healthcare advisory perspective, the reported 42.5% clinical pregnancy rate, 27.5% live birth rate, and NNT values of 4 and 5 represent clinically meaningful findings for carefully selected patients with repeated implantation failure and elevated Th1/Th2 ratios. However, healthcare organizations should avoid interpreting one well-designed randomized trial as sufficient justification for universal implementation across all IVF programs. Evidence-based reproductive medicine requires balancing promising efficacy data against patient selection, long-term safety, operational feasibility, and healthcare economics.
The first limitation is study size because only 80 patients completed randomization despite 153 patients initially undergoing screening. Although statistical significance was achieved, relatively small sample sizes increase uncertainty around treatment effect estimates and widen confidence intervals. The reported 95% confidence interval for live birth (1.21–11.63) illustrates that while benefit is likely, the exact magnitude remains uncertain until confirmed in larger multicenter studies.
Another important consideration is population specificity. Only women demonstrating a Th1/Th2 ratio of at least 10.3 were eligible, meaning nearly 40% of screened patients were excluded before randomization or through subsequent eligibility criteria. Consequently, these results should not be generalized to all women experiencing implantation failure because immune dysfunction represents only one component of a multifactorial reproductive disorder.
Repeated implantation failure itself remains clinically heterogeneous. International fertility literature identifies embryo aneuploidy, maternal age, diminished ovarian reserve, chronic endometritis, uterine anomalies, endometrial receptivity disorders, thrombophilia in selected patients, endocrine abnormalities, obesity, adenomyosis, and lifestyle factors as additional contributors to implantation failure. An immunosuppressive strategy cannot compensate for poor embryo quality, uncontrolled endocrine disease, or structural uterine pathology.
Embryo genetics continue to represent one of the strongest determinants of implantation success. Human embryos demonstrate relatively high rates of chromosomal abnormalities, particularly as maternal age increases beyond 35 years, with aneuploidy prevalence rising substantially during later reproductive years. Even complete normalization of maternal immune responses cannot consistently overcome implantation failure if transferred embryos possess significant chromosomal abnormalities.
Carethix also identifies operational challenges for fertility centers considering immune-guided treatment pathways. Standardizing cytokine testing, laboratory calibration, assay reproducibility, reporting thresholds, physician interpretation, and quality assurance requires additional clinical governance infrastructure. Without standardized laboratory protocols, identical patients may receive different clinical decisions simply because immune biomarker testing lacks universal international harmonization.
Economic considerations deserve equal attention. IVF treatment already represents a substantial financial burden. Additional immune investigations, repeated cytokine testing, specialist consultations, and immunomodulatory medications increase total treatment expenditure. Healthcare organizations therefore need cost-effectiveness analyses demonstrating whether improved live birth rates offset additional diagnostic and therapeutic costs across larger patient populations.
Safety evaluation should extend well beyond short-term treatment tolerance. Tacrolimus has been used extensively within organ transplantation, but fertility treatment introduces different clinical objectives involving embryo development, placental biology, fetal growth, neonatal outcomes, and long-term child health. Although no severe adverse events occurred during this trial, larger datasets involving several hundred or several thousand pregnancies would provide greater confidence regarding rare complications.
Another strategic gap involves treatment duration. Patients received tacrolimus for only 16 days, beginning 2 days before embryo transfer and continuing until pregnancy testing. Important questions remain regarding optimal dosage, therapeutic drug monitoring, treatment continuation after positive pregnancy tests, discontinuation strategies, and interactions with progesterone, estrogen supplementation, anticoagulation protocols, and other fertility medications.
Clinical implementation also requires multidisciplinary collaboration rather than isolated prescribing decisions. Reproductive endocrinologists, fertility specialists, reproductive immunologists, maternal-fetal medicine physicians, pharmacists, embryologists, laboratory scientists, and nursing teams should collectively evaluate immune-directed treatment eligibility. This integrated governance model reduces inappropriate prescribing while strengthening patient safety and clinical accountability.
The trial nevertheless represents an important milestone because it moves reproductive immunology toward higher-quality evidence. Historically, several adjunctive fertility therapies entered clinical practice with limited randomized evidence, creating uncertainty regarding effectiveness and resource utilization. By contrast, randomized, double-blind, placebo-controlled methodology establishes a stronger foundation for future guideline development even if additional validation remains necessary.
Carethix believes the greatest value of this research lies in reinforcing precision medicine rather than expanding empirical immunotherapy. Fertility care increasingly depends on identifying measurable biological abnormalities before selecting targeted interventions instead of relying on generalized treatment algorithms. This philosophy supports better clinical governance, improved patient counseling, more efficient healthcare spending, and higher-value reproductive medicine capable of delivering measurable outcomes while maintaining patient safety.
Carethix Solutions: Building a Precision Immunology Framework for Better Pregnancy Outcomes
Carethix recommends that fertility centers move from empirical treatment toward a structured precision reproductive medicine model supported by measurable clinical indicators. The recent randomized trial demonstrated a 42.5% clinical pregnancy rate, 27.5% live birth rate, 27.5% absolute improvement in clinical pregnancy, and an NNT of only 4, but these benefits were achieved only after identifying women with a documented Th1/Th2 ratio ≥10.3. The primary lesson is not that every RIF patient requires tacrolimus, but that every patient deserves a comprehensive diagnostic pathway before therapeutic decisions are made.
The first strategic priority should be comprehensive patient stratification before embryo transfer. Every repeated implantation failure case should undergo systematic evaluation covering maternal age, embryo quality, chromosomal assessment where appropriate, uterine cavity evaluation, endocrine disorders, chronic endometritis, metabolic disease, thrombosis risk when clinically indicated, autoimmune history, and immune biomarkers. Structured diagnostic algorithms reduce unnecessary treatments while improving clinical consistency across fertility programs.
Healthcare organizations should establish standardized reproductive immunology protocols supported by accredited laboratory services. Cytokine measurements, Th1/Th2 ratio analysis, laboratory calibration, quality control procedures, specimen handling, turnaround time, and reporting standards should be governed through documented operating procedures. Standardization improves reproducibility while minimizing diagnostic variation between different fertility centers.
A multidisciplinary fertility board should review complex implantation failure cases before introducing immunomodulatory therapy. Reproductive endocrinologists, reproductive immunologists, embryologists, maternal-fetal medicine specialists, clinical pharmacists, laboratory physicians, nurses, and quality managers each contribute unique expertise that strengthens patient selection. Multidisciplinary governance reduces inappropriate prescribing while improving clinical safety and documentation quality.
Embryo quality optimization should remain the highest clinical priority because implantation begins with embryo competence. Blastocyst culture optimization, laboratory quality indicators, embryo grading systems, incubator performance monitoring, contamination control, air quality management, and evidence-based embryo transfer practices directly influence reproductive outcomes. Even the most effective immunotherapy cannot consistently compensate for poor embryo viability.
Healthcare providers should also optimize endometrial health before transfer cycles. Three-dimensional ultrasound, hysteroscopy when indicated, assessment of uterine pathology, treatment of chronic endometritis, management of fibroids affecting the uterine cavity, correction of intrauterine adhesions, and evaluation of endometrial thickness collectively improve implantation conditions. Addressing structural abnormalities before immunotherapy increases the likelihood that biological improvements translate into successful pregnancies.
Patient counseling must become more data-driven. Rather than offering generalized optimism, clinicians should explain that the recent study included 80 randomized patients, demonstrated 17 clinical pregnancies versus 6, and achieved 11 live births versus 3 among carefully selected participants. Presenting absolute risk differences, relative risks, confidence intervals, and Number Needed to Treat enables patients to make informed decisions based on measurable evidence instead of unrealistic expectations.
Medication safety monitoring should accompany every immunosuppressive protocol. Baseline laboratory investigations, liver function assessment, renal function monitoring, infection screening, medication reconciliation, adverse event reporting, and standardized follow-up visits reduce preventable complications. Digital clinical dashboards can further improve monitoring by tracking treatment adherence, laboratory trends, and pregnancy outcomes throughout the IVF cycle.
Healthcare organizations should implement prospective outcome registries for every immune-directed fertility intervention. Clinical pregnancy, biochemical pregnancy, implantation rate, miscarriage, live birth, neonatal outcomes, maternal complications, medication adverse events, and patient-reported outcomes should all be captured in standardized databases. Registry-based evidence strengthens institutional quality improvement while generating valuable real-world clinical evidence beyond randomized trials.
Artificial intelligence and predictive analytics also represent emerging opportunities within fertility medicine. Machine learning models integrating maternal demographics, ovarian reserve markers, embryo morphology, cytokine profiles, endocrine variables, previous IVF history, and immunological biomarkers may improve prediction of implantation success. These technologies should support clinical judgment rather than replace physician decision-making, ensuring transparency and patient-centered care.
Healthcare leadership should also evaluate financial sustainability before implementing advanced reproductive immunology services. Cost-effectiveness analyses should compare additional laboratory expenses against reductions in repeated IVF cycles, fewer failed embryo transfers, lower emotional burden, and improved cumulative live birth rates. Value-based reproductive medicine requires demonstrating measurable clinical benefit alongside responsible resource utilization.
Finally, research investment should remain a strategic priority. Large multicenter randomized trials involving several hundred or several thousand patients across different ethnic groups, healthcare systems, and IVF laboratories are needed to validate current findings. Future studies should also investigate optimal tacrolimus dosing, duration of therapy, long-term maternal safety, neonatal outcomes, pharmacogenomics, immune biomarkers beyond Th1/Th2 ratios, and comparative effectiveness against other evidence-based fertility interventions.
Carethix believes the future of reproductive medicine will not be defined by broader use of immunosuppressants alone. Instead, success will come from integrating precision diagnostics, multidisciplinary governance, standardized laboratory medicine, evidence-based pharmacotherapy, digital quality management, continuous outcome measurement, and patient-centered clinical decision-making. Fertility centers that invest in these integrated capabilities will be better positioned to improve implantation success, increase live birth rates, strengthen healthcare quality, and deliver sustainable long-term value for patients and healthcare systems alike.
Future Prevention: Strengthening Long-Term Governance for Immune-Guided Fertility Care
Carethix advises healthcare organizations to treat the recent tacrolimus trial as a catalyst for strengthening reproductive governance rather than as a standalone therapeutic solution. The study demonstrated a 42.5% clinical pregnancy rate, 27.5% live birth rate, a 27.5% absolute improvement in clinical pregnancy, and a 20.0% absolute improvement in live birth, yet sustained success depends on preventing inappropriate patient selection, inconsistent laboratory practices, and fragmented clinical pathways. Long-term reproductive quality requires healthcare systems to standardize diagnostics, clinical decision-making, and continuous performance evaluation.
The first prevention strategy is establishing standardized diagnostic criteria for repeated implantation failure across every fertility center. Variations in RIF definitions continue to create inconsistent patient populations between clinical studies and healthcare organizations, making outcome comparisons difficult. Standardized eligibility criteria improve research quality, clinical benchmarking, and treatment consistency while reducing unnecessary exposure to immunosuppressive therapies.
Healthcare systems should adopt mandatory immune biomarker validation before initiating immune-directed interventions. Patients should demonstrate objective laboratory evidence of immune dysregulation, including validated cytokine testing and standardized Th1/Th2 ratio assessment, before immunomodulatory medications are prescribed. Evidence-driven prescribing minimizes overtreatment while directing healthcare resources toward patients most likely to benefit.
Quality assurance programs should monitor every stage of laboratory performance. Internal quality control, external proficiency testing, equipment calibration, specimen traceability, reagent validation, and regular laboratory audits reduce analytical variability that could influence treatment decisions. Reliable laboratory medicine forms the foundation of precision reproductive healthcare because inaccurate immune testing can lead directly to inappropriate clinical management.
Fertility centers should establish prospective clinical registries tracking every immune-guided treatment cycle. Standardized reporting should include implantation rate, biochemical pregnancy, clinical pregnancy, ongoing pregnancy, miscarriage, preterm birth, live birth, congenital anomalies, maternal complications, neonatal outcomes, and long-term child development. Large longitudinal databases generate higher-quality evidence than isolated institutional experience and accelerate continuous quality improvement.
Medication safety surveillance should continue throughout pregnancy whenever clinically appropriate. Although the randomized trial reported no severe adverse events and no treatment discontinuations, larger patient populations are required to identify uncommon maternal or fetal complications that may occur at frequencies below 1%. Pharmacovigilance systems therefore remain essential components of responsible reproductive healthcare governance.
Healthcare organizations should strengthen infection prevention protocols before prescribing immunosuppressive medications. Comprehensive medical history, vaccination review where appropriate, infectious disease assessment, medication interaction screening, and individualized risk stratification reduce preventable complications associated with temporary immune modulation. Preventive medicine remains more effective and less costly than managing avoidable adverse clinical events after treatment initiation.
Digital healthcare technologies should become essential components of reproductive medicine quality management. Electronic clinical pathways, automated laboratory alerts, medication reconciliation systems, adverse event reporting platforms, patient engagement applications, and real-time outcome dashboards improve transparency while reducing administrative variation. Digital quality infrastructure also enables fertility centers to benchmark performance against national and international quality indicators.
Continuous clinician education represents another essential prevention strategy. Fertility specialists, embryologists, nurses, reproductive immunologists, pharmacists, laboratory scientists, and quality managers should receive regular updates on emerging randomized evidence, evolving clinical guidelines, immune biomarkers, medication safety, and personalized fertility care. Healthcare knowledge evolves rapidly, making structured continuing professional development a critical investment rather than an optional activity.
Patient education should receive equal emphasis because informed patients participate more effectively in shared clinical decision-making. Counseling should clearly explain that the trial included 80 randomized participants, demonstrated statistically significant improvements within a narrowly defined immune subgroup, and does not establish tacrolimus as a universal therapy for infertility. Transparent communication improves treatment adherence while reducing unrealistic expectations and decision regret.
Future clinical research should prioritize larger international multicenter trials involving diverse ethnic populations, multiple healthcare systems, and different IVF laboratory environments. Studies involving 500 to 2,000 participants would provide substantially greater statistical precision, strengthen subgroup analyses, and improve understanding of long-term maternal and neonatal safety. Comparative effectiveness research should also evaluate tacrolimus against other evidence-based adjunctive therapies while incorporating health economic analyses and quality-of-life outcomes.
Carethix Key Takeaway
Carethix believes this randomized trial represents one of the more meaningful advances in immune-guided reproductive medicine because it demonstrated measurable improvements across clinically important outcomes, including a 42.5% clinical pregnancy rate, a 27.5% live birth rate, an NNT of 4 for clinical pregnancy, an NNT of 5 for live birth, and a statistically significant reduction in the Th1/Th2 ratio from 17.01 to 12.56. These results support further integration of precision immunology into fertility care, but only for carefully selected patients supported by objective laboratory evidence and multidisciplinary clinical oversight.
The larger message extends beyond tacrolimus itself. Modern fertility medicine should move away from empirical interventions and toward biomarker-driven clinical pathways that integrate reproductive immunology, embryo quality assessment, advanced laboratory diagnostics, digital quality management, pharmacovigilance, and continuous outcome measurement. Healthcare organizations that combine these capabilities will be better positioned to improve implantation success, increase cumulative live birth rates, optimize healthcare resource utilization, strengthen patient safety, and deliver sustainable value across the rapidly evolving landscape of reproductive medicine.

