
Norovirus outbreaks reached a 3.3% infection rate on cruises, highlighting urgent guest safety and infection control needs.
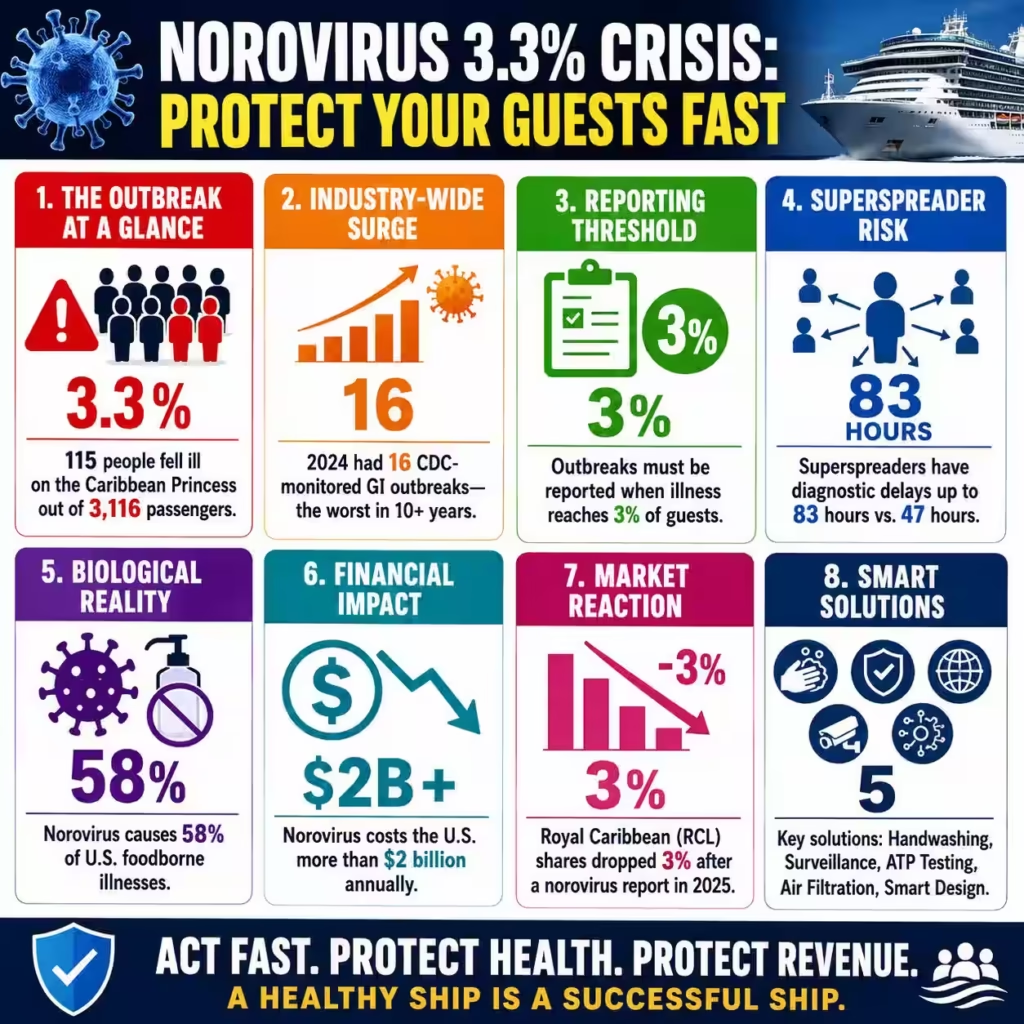
The Caribbean Princess cruise ship reported that 102 passengers and 13 crew members fell ill with norovirus during its voyage from Port Everglades, representing a critical 3.3% infection rate among 3,116 passengers. This outbreak, occurring between April 28 and May 11, highlights a recurring vulnerability in the $18.8 billion cruise industry where high population density accelerates viral transmission. Our analysis indicates that the economic burden of norovirus in the United States exceeds $2 billion annually, primarily driven by lost productivity and immediate healthcare interventions.
Historical data suggests that such outbreaks are not isolated, as 2024 was recorded as the worst year for maritime gastrointestinal illnesses in over a decade with 16 reported CDC-monitored incidents. The Caribbean Princess incident follows a similar outbreak on the Star Princess in March, where 153 individuals were sickened, signaling a systemic failure in current containment strategies. This trend suggests that current sanitization protocols are insufficient against GII.4 Sydney, the dominant and highly resilient viral strain currently circulating globally.
Beyond the immediate health risk, the Caribbean Princess outbreak serves as a stark reminder of the financial volatility inherent in mass-market tourism. When a ship reports a 3% illness threshold, it triggers mandatory CDC Vessel Sanitation Program (VSP) intervention, often resulting in expensive field responses and environmental assessments. The industry faces an uphill battle as 2025 has already seen 19 major gastrointestinal outbreaks, 14 of which are laboratory-confirmed norovirus cases.
From a B2B perspective, the Caribbean Princess event underscores the “superspreader” phenomenon, where a small percentage of infected individuals contribute to the majority of secondary cases. Reconstructed transmission chains in similar maritime outbreaks reveal that superspreaders often exhibit diagnostic delays of up to 83 hours, compared to the 47-hour average for typical cases. This lag time allows the virus to permeate high-touch surfaces in communal dining areas and shared ventilation corridors before isolation protocols are even activated.
Princess Cruises responded by isolating ill individuals and increasing disinfection, but these reactive measures often failed to stop the initial surge of the 12 to 48-hour incubation period. Professional consultancy firms now advise cruise operators to integrate real-time bio-surveillance to identify early symptomatic clusters before they reach the 3% reporting threshold. Strategic recovery requires more than increased cleaning; it demands a total overhaul of digital health tracking and guest screening technologies.
Strong Critique of Maritime Health Gaps and Operational Risks
The current response by Princess Cruises and the broader maritime sector is fundamentally reactive, addressing symptoms rather than the systemic architectural flaws that facilitate viral spread. While the CDC mandates reporting at the 3% threshold, this metric is a lagging indicator that allows the virus to achieve deep saturation within the vessel’s biome. By the time 115 people are symptomatic, thousands more have likely been exposed through aerosolized viral particles and contaminated high-touch points.
Carethix views the reliance on manual guest reporting as a critical operational risk, as passengers often hide symptoms to avoid cabin isolation and missed excursions. This behavioral gap creates a “shadow caseload” that sabotages even the most rigorous environmental cleaning schedules. Furthermore, the maritime industry’s heavy reliance on alcohol-based hand sanitizers represents a significant technical gap in infection control.
Norovirus is a non-enveloped virus, making it notoriously resistant to standard hand sanitizers that are highly effective against lipid-enveloped viruses like Influenza or SARS-CoV-2. The “sanitizer-first” culture on cruise ships provides a false sense of security while doing little to neutralize the primary pathogen responsible for 58% of U.S. foodborne illnesses. Carethix critiques the lack of mandatory, supervised hand-washing stations at all dining entrances, which remains the only proven method for mechanical removal of the virus.
Failure to address this specific biological reality results in predictable, recurring outbreaks that damage brand equity and drive down stock valuations. The financial fallout of these incidents extends far beyond the immediate voyage, impacting long-term consumer confidence and increasing insurance premiums. In 2025, Royal Caribbean (RCL) saw shares drop by 3% immediately following a norovirus report, illustrating the market’s sensitivity to maritime health stability.
These outbreaks often lead to litigation, costly mid-voyage itinerary changes, and the need for expensive deep-cleaning “gap days” between sailings. The current “isolate and clean” model is an antiquated approach that fails to account for the velocity of modern viral variants. Carethix asserts that without a transition to proactive, technology-driven health architectures, cruise lines will continue to experience these multi-million dollar revenue leaks.
| Related Analysis: AI 81% Adoption Risk Crisis: Boost Your Cash Flow 64% Denial Risk Exposure: Defend Your Revenue Today Hantavirus 40% Mortality Crisis: Your Safer Fleet Model |
Comprehensive Solutions for Maritime Infection Control
To mitigate the $60 billion global economic impact of norovirus, cruise operators must pivot from manual protocols to automated, AI-driven health monitoring systems. Implementing IoT-enabled soap dispensers and “smart” hand-washing stations can provide real-time data on guest and crew compliance, allowing for targeted interventions in specific ship zones. These systems can alert management when compliance drops below a predetermined safety threshold, enabling corrective action before an outbreak begins.
Furthermore, the integration of ATP (Adenosine Triphosphate) testing for surface cleanliness offers an objective, data-driven alternative to visual inspections. By quantifying microbial loads on high-touch surfaces, crews can optimize cleaning schedules based on actual risk rather than arbitrary time intervals. Investment in advanced HVAC filtration and UV-C light disinfection technologies is another essential B2B solution for high-density environments.
Research indicates that norovirus can become aerosolized during vomiting incidents, allowing for rapid spread through shared ventilation systems. Installing medical-grade HEPA filters and Far-UVC 222nm lamps in common areas can neutralize pathogens in the air and on surfaces without harming human skin or eyes. These technological upgrades transform the ship’s physical environment into a proactive shield, reducing the burden on cleaning crews and minimizing human error.
Professional healthcare consultants recommend these capital expenditures as high-ROI investments that protect the fleet’s operational continuity and long-term brand reputation. Finally, cruise lines must reform their guest and crew medical policies to incentivize early symptom reporting and transparent health disclosure. This includes offering “isolation credits” or travel vouchers for passengers who report illness early and follow quarantine, effectively removing the financial penalty for honesty.
For crew members, strict “no-fault” sick leave policies are non-negotiable to prevent infected food handlers from triggering mass-casualty events. These behavioral economics solutions address the human element of viral transmission, which is often the weakest link in the safety chain. By aligning guest incentives with public health goals, operators can significantly flatten the infection curve during the critical 12-hour incubation window.
Prevention Steps for Future Fleet Health Integrity
Future-proofing the cruise industry against norovirus requires a fundamental shift toward “Health by Design” in ship architecture and operational workflows. New vessel builds should prioritize non-porous, antimicrobial materials for all high-touch surfaces, including railings, elevator buttons, and buffet counters. Copper-alloy surfaces or specialized antimicrobial coatings can provide continuous passive protection, reducing the environmental reservoir of the virus.
Additionally, the move away from traditional self-service buffets to “crew-served” dining models significantly reduces the risk of cross-contamination via shared utensils. These structural changes minimize the number of common touchpoints, making it exponentially harder for a single infected individual to seed a ship-wide outbreak. Continuous education and rigorous certification programs for crew members must be standardized across the global fleet to ensure a baseline of health literacy.
Training should move beyond basic sanitation to include advanced epidemiological principles, such as understanding viral shedding durations and aerosolization risks. Regular, unannounced audits of VSP protocols by third-party healthcare consultants can identify “blind spots” in a ship’s defense before the CDC arrives for a formal inspection. These audits should include environmental swabbing and review of medical log accuracy to ensure that early-warning signs are not being overlooked.
Maintaining a “culture of clinical excellence” among the crew is the most effective defense against the introduction of pathogens from shore-side excursions. Lastly, the industry must collaborate on a shared “Global Maritime Health Database” to track viral trends and emerging strains in real-time across different lines. This B2B data-sharing initiative would enable operators to anticipate regional surges in norovirus activity and implement “Level 2” precautions before a ship even enters a high-risk port.
By treating maritime health as a collective security issue rather than a competitive secret, the industry can raise the standard for all players. Proactive collaboration with port authorities to ensure the hygiene of shore-side water supplies and food vendors is equally critical. These multi-layered prevention strategies ensure that the next Caribbean Princess voyage remains defined by luxury rather than laboratory-confirmed gastroenteritis.
Key Takeaway: The Carethix Executive Mandate
The Caribbean Princess outbreak is not a fluke; it is a predictable outcome of prioritizing aesthetic luxury over clinical-grade operational resilience. If you are an executive in the maritime space, you must recognize that a 3.3% infection rate is a failure of your current bio-security infrastructure. Reactive cleaning is a PR exercise, not a medical strategy; you need real-time surveillance and mechanical viral removal to survive the next norovirus season.
Stop relying on alcohol gels and start investing in smart-wash technology and air-purification systems that actually neutralize non-enveloped viruses. Your brand’s financial health is inextricably linked to your fleet’s biological health—act now or prepare for the next CDC headline. Implement these clinical standards today to secure your revenue and protect your passengers from preventable medical crises.
FAQs:
Why did the 3.3% norovirus outbreak on the Caribbean Princess escalate to 115 infections despite existing sanitation protocols?
Reactive “clean-after-outbreak” models are insufficient because a virus with a 12–48 hour incubation period can disseminate through communal dining areas and ventilation systems before isolation protocols can be effectively implemented.
How does the $2 billion annual U.S. norovirus burden expose critical weaknesses in cruise ship infection-control systems?
The industry still over-relies on alcohol sanitizers and manual symptom reporting instead of deploying AI-driven bio-surveillance and mechanical viral-removal infrastructure.
Why are 2025’s 19 major gastrointestinal outbreaks a serious operational risk for the $18.8 billion cruise industry?
Repeated CDC-monitored outbreaks reveal systemic biosecurity underinvestment that threatens revenue continuity, brand trust, and long-term passenger confidence.
How can cruise operators reduce the 83-hour superspreader diagnostic delay linked to rapid norovirus transmission?
Operators must replace passive guest self-reporting with real-time health analytics, smart compliance tracking, and proactive symptom-detection systems.
Why did Royal Caribbean’s 3% stock decline after a norovirus report signal broader investor concerns about maritime health resilience?
Markets increasingly view recurring outbreak headlines as evidence of outdated operational architecture that creates preventable multimillion-dollar revenue leakage.

