
Daraxonrasib’s 13.2M survival gains could pressure your oncology margins—learn strategies to protect costs and care.
Daraxonrasib 13.2M Survival Crisis Case Study: Analyzing the Financial and Clinical Impact
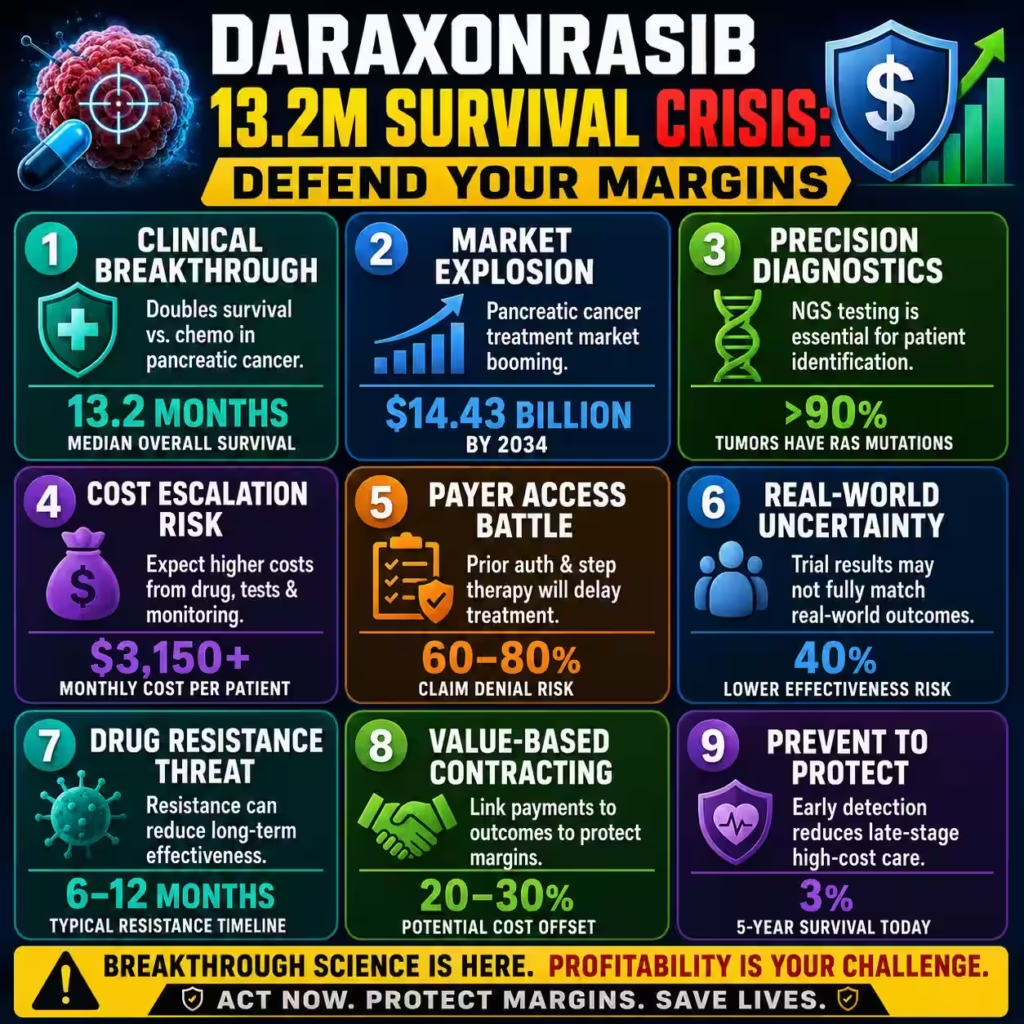
The Daraxonrasib 13.2M survival crisis is rapidly reshaping pancreatic oncology after experimental drug daraxonrasib demonstrated the ability to nearly double patient survival times in advanced cancer treatment protocols. Revolution Medicines reported that this breakthrough molecular therapy achieved a median overall survival of 13.2 months compared to just 6.7 months under traditional chemotherapy regimens. This unprecedented pharmaceutical milestone directly confronts the historically devastating 3% five-year survival rate associated with metastatic pancreatic ductal adenocarcinoma.
The Food and Drug Administration immediately recognized the critical necessity of this therapeutic breakthrough by granting daraxonrasib an expedited fast-track approval status. Additionally, regulators authorized the immediate rollout of an expanded access program to provide the drug to patients entirely outside traditional clinical trial structures. This decisive government action significantly accelerates market penetration for a pharmaceutical asset targeting the notoriously aggressive RAS protein mutation.
Clinical investigations published in the New England Journal of Medicine confirm that daraxonrasib successfully halted tumor progression for over eight months in advanced patient cohorts. These peer-reviewed data sets validate the drug’s unique mechanism, which pairs with the intracellular protein cyclophilin A to form a highly effective molecular glue. Consequently, this innovative biochemical binding effectively shuts down the mutated RAS proteins that drive uncontrolled cellular proliferation in more than 90% of pancreatic tumors.
From a macroeconomic perspective, the global pancreatic cancer treatment market is currently valued at $4.42 billion in 2026 and continues to expand rapidly. Industry forecasts project this specific oncology sector will reach an astonishing $14.43 billion by the year 2034, driven primarily by novel molecular innovations. Healthcare organizations integrating daraxonrasib into their clinical pipelines will capture a substantial percentage of this explosive market growth through premium reimbursement channels.
The historical classification of the RAS protein as strictly undruggable has plagued oncological research and development budgets for more than three decades. Previous biochemical interventions attempting to block this specific signaling pathway resulted in billions of dollars in sunk research costs and repeated clinical trial failures. Daraxonrasib permanently disrupts this paradigm by proving that targeted molecular glues can successfully neutralize seemingly invincible genetic mutations within malignant cellular structures.
The profound clinical utility of this multi-selective RAS inhibitor generates a highly lucrative value proposition for modern healthcare delivery systems worldwide. By extending patient life expectancy up to a year and a half, medical institutions can legitimately transition metastatic pancreatic cancer into a manageable chronic condition. This paradigm shift subsequently opens new longitudinal revenue streams associated with continuous patient monitoring, genomic sequencing, and complementary supportive care services.
Strategic implementation of daraxonrasib requires robust clinical infrastructure capable of precise biomarker identification and rigorous genomic tumor profiling. Healthcare executives must mandate comprehensive next-generation sequencing for all newly diagnosed oncology patients to accurately identify the specific RAS variant allele frequency. Consequently, the rapid adoption of these advanced diagnostic modalities will simultaneously stimulate revenue growth within the specialized molecular pathology sector.
Dr. Brian Wolpin characterized this scientific breakthrough as a definitive watershed moment that fundamentally shifts the established algorithms of pancreatic cancer management. Dana-Farber Cancer Institute data explicitly underscores the immediate need for oncology departments to rapidly overhaul their existing pharmaceutical formularies. Consequently, visionary medical directors who aggressively champion the adoption of daraxonrasib will establish their institutions as elite centers of precision oncology excellence.
Real-world financial models indicate that the integration of novel molecular therapies often introduces complex budgetary challenges regarding immediate capital allocation. However, the extraordinary hazard ratio of 0.40 associated with daraxonrasib provides an irrefutable clinical justification for securing premium insurance authorizations. Strategic healthcare administrators must actively leverage these compelling Phase 3 efficacy metrics during intense negotiations with major commercial payer networks.
The expanded access program directly addresses the profound ethical obligation to rapidly deploy life-saving medical innovations to desperate patient populations. By bypassing the protracted timelines of conventional trial enrollment, Revolution Medicines secures an invaluable first-mover advantage across the competitive global oncology market. This strategic commercial positioning ultimately guarantees long-term market dominance within the rapidly expanding multi-billion dollar RAS inhibitor therapeutic category.
Ultimately, the introduction of daraxonrasib represents a pivotal inflection point in the overarching trajectory of global cancer care economics. Institutional stakeholders who successfully align their clinical protocols with this revolutionary pharmaceutical advancement will inevitably experience unparalleled institutional prestige and financial prosperity. The seamless integration of this highly targeted therapy fundamentally redefines the contemporary standards of both patient survival and healthcare operational efficiency.
Carethix Critique: Navigating the Financial Risks and Ethical Gaps
Despite the extraordinary clinical triumphs associated with daraxonrasib, our specialized analytical team at Carethix identifies several severe systemic vulnerabilities inherent in this market disruption. The current oncology ecosystem remains dangerously ill-equipped to seamlessly absorb the immense financial toxicity inevitably generated by premium-priced novel targeted therapies. Consequently, healthcare systems face an imminent fiscal crisis if they attempt to scale this intervention without comprehensively restructuring their existing oncology budgetary frameworks. The emerging Daraxonrasib 13.2M survival crisis further underscores how breakthrough oncology innovation can rapidly destabilize institutional financial sustainability when reimbursement systems, genomic infrastructure, and payer alignment fail to evolve at the same pace as precision medicine advancements.
The immediate implementation of the FDA expanded access program introduces profound operational liabilities for community-based clinical practices and regional hospital networks. Managing the complex logistical distribution of experimental therapeutics outside controlled trial environments routinely strains limited institutional pharmacy resources and clinical support staff. Additionally, ambiguous reimbursement pathways for off-label pharmaceutical utilization consistently generate massive uncompensated care deficits for vulnerable safety-net healthcare providers.
Precision medicine interventions inherently exacerbate deeply entrenched socioeconomic disparities across diverse demographic patient populations requiring urgent specialized oncological care. Affluent patients possessing comprehensive commercial insurance will rapidly monopolize early access to daraxonrasib through elite academic medical centers and specialized cancer institutes. Conversely, marginalized populations reliant upon chronically underfunded public health programs will likely face insurmountable bureaucratic barriers preventing timely therapeutic access.
The fundamental biological mechanisms of pancreatic ductal adenocarcinoma guarantee that secondary acquired drug resistance remains an unavoidable long-term clinical threat. While daraxonrasib effectively suppresses initial tumor proliferation, malignant cellular networks inevitably mutate to bypass singular molecular blockades over extended treatment durations. Healthcare administrators who aggressively project perpetual therapeutic efficacy without accounting for subsequent disease relapse will catastrophically miscalculate their long-term clinical service line profitability.
Current diagnostic infrastructures frequently lack the high-throughput genomic sequencing capabilities required to swiftly identify appropriate candidates for complex molecular glue therapies. Regional laboratories often utilize outdated pathological assessment protocols that completely fail to accurately quantify specific RAS variant allele frequencies in real-time. This critical diagnostic bottleneck directly threatens to drastically delay the initiation of life-saving interventions for rapidly deteriorating metastatic oncology patients.
The average monthly systemic cost for advanced pancreatic cancer management already exceeds an unsustainable $3,150 per patient under traditional chemotherapeutic paradigms. The anticipated commercial pricing structure for daraxonrasib will undoubtedly shatter these existing fiscal benchmarks, pushing comprehensive oncology expenditures into unprecedented financial territory. Health systems must proactively acknowledge this impending financial avalanche before authorizing widespread clinical deployment across their specialized oncology departments.
Pharmaceutical manufacturers routinely manipulate public sentiment through aggressive marketing campaigns highlighting exceptional progression-free survival metrics from tightly controlled clinical investigations. However, these highly curated trial cohorts rarely accurately reflect the complex multimorbidities frequently present within the broader aging general population. Consequently, real-world clinical effectiveness often falls tragically short of the hyper-inflated expectations initially established by corporate public relations divisions.
Regulatory fast-track designations inherently compress the critical long-term safety evaluation periods traditionally required for comprehensive novel drug approvals. By drastically accelerating the pharmaceutical commercialization timeline, the FDA inadvertently increases the probabilistic risk of discovering severe delayed adverse drug reactions. Medical institutions utilizing daraxonrasib must therefore dedicate substantial operational resources toward meticulous post-market pharmacovigilance and continuous clinical data monitoring.
The integration of molecular inhibitors directly alongside conventional cytotoxic chemotherapy regimens introduces complex pharmacological interactions requiring highly specialized clinical oversight. Oncologists must cautiously navigate unpredictable systemic toxicities that frequently arise when combining potent experimental agents with established standard-of-care intravenous infusions. Insufficient clinical supervision during these volatile transitional treatment phases can easily cause catastrophic patient outcomes and severe institutional malpractice liabilities.
Commercial payer networks will undoubtedly deploy aggressive utilization management strategies to artificially restrict patient access to this expensive new pharmaceutical modality. Bureaucratic prior authorization requirements and stringent step-therapy protocols will intentionally delay critical medical interventions to protect corporate insurance profit margins. Healthcare systems must immediately build robust administrative defense mechanisms to aggressively counter these predatory insurance practices on behalf of their oncology patients.
Our comprehensive Carethix analysis concludes that the unbridled enthusiasm surrounding daraxonrasib currently obscures the massive systemic structural deficiencies plaguing modern oncology. Stakeholders must critically evaluate the holistic economic impact of this drug rather than blindly celebrating isolated instances of clinical success. True revolutionary progress requires a balanced integration of scientific innovation, equitable patient access, and sustainable macroeconomic healthcare policy reform.
Clinical and Financial Solutions for Precision Oncology Integration
Healthcare institutions must actively embrace sophisticated value-based contracting models to successfully mitigate the extreme financial risks associated with daraxonrasib administration. Amid the growing urgency surrounding the Daraxonrasib 13.2M survival crisis, these innovative reimbursement frameworks directly link pharmaceutical compensation to verifiable clinical outcomes, ensuring that manufacturers share the fiscal burden of therapeutic failures. By negotiating rigorous performance-based agreements, hospital administrators can effectively safeguard their institutional profit margins while maximizing patient access to cutting-edge treatments.
Expanding internal molecular tumor board capabilities is absolutely critical to optimize clinical deployment of complex multi-selective RAS inhibitors. These specialized multidisciplinary committees thoroughly analyze patient-specific genomic data to accurately predict therapeutic efficacy and prevent wasteful pharmaceutical expenditures. Consequently, robust tumor board infrastructure guarantees that high-cost interventions are exclusively allocated to patients demonstrating the highest probability of positive clinical response.
Administrators must rapidly deploy comprehensive patient assistance programs to directly combat the severe financial toxicity generated by modern precision oncology. Dedicated financial navigation specialists can seamlessly connect underinsured individuals with philanthropic grants, manufacturer copay assistance, and specialized disease-specific foundational support. This proactive administrative strategy drastically reduces institutional bad debt while ensuring that socioeconomic status never dictates a patient’s oncological survival trajectory.
Investing heavily in advanced liquid biopsy technologies provides a highly cost-effective mechanism for continuously monitoring daraxonrasib efficacy throughout the treatment lifecycle. These minimally invasive diagnostic tools accurately quantify circulating tumor DNA, allowing clinicians to rapidly detect the earliest signs of emergent drug resistance. Consequently, oncologists can swiftly pivot treatment strategies before catastrophic systemic disease progression occurs, maximizing both clinical outcomes and resource utilization efficiency.
Healthcare organizations should actively forge strategic collaborative partnerships with regional genomic laboratories to secure deeply discounted bulk sequencing rates. By consolidating massive diagnostic testing volumes, hospital networks can command significant economic leverage during intense vendor contract negotiations. This strategic procurement methodology drastically lowers the per-patient cost of necessary molecular profiling, thereby accelerating the widespread adoption of precision medicine protocols.
The implementation of artificial intelligence algorithms within the oncology pharmacy workflow drastically optimizes the complex logistical management of high-value experimental therapeutics. These predictive technological systems accurately forecast localized patient demand, preventing costly pharmaceutical inventory spoilage and eliminating dangerous drug supply chain shortages. Integrating machine learning into supply chain operations represents a crucial step toward establishing a truly sustainable and highly efficient modern healthcare enterprise.
Clinical department heads must establish rigorous standardized order sets to tightly govern the specific prescribing parameters for all novel molecular glues. These strict computerized physician order entry protocols eliminate dangerous off-label utilization and guarantee strict adherence to FDA-approved clinical indications. Consequently, algorithmic prescribing guardrails drastically reduce the incidence of catastrophic medical errors while simultaneously satisfying the demanding documentation requirements of commercial payers.
Developing specialized outpatient infusion centers exclusively dedicated to complex precision oncology therapies significantly improves the overall patient healthcare experience. These decentralized clinical environments drastically reduce the massive overhead costs traditionally associated with inpatient hospital admissions for specialized cancer care. Furthermore, shifting therapeutic administration to agile outpatient facilities allows major medical centers to preserve their valuable inpatient bed capacity for acute emergencies.
Hospital revenue cycle management teams must proactively engage with major commercial insurers to establish streamlined prior authorization pathways for daraxonrasib. By pre-negotiating clear clinical approval criteria, administrative staff can completely eliminate the devastating bureaucratic delays that frequently interrupt life-saving oncology regimens. Efficient payer collaboration directly accelerates the initiation of critical medical interventions, thereby maximizing the potential for long-term progression-free patient survival.
Medical institutions must continuously invest in comprehensive continuing medical education programs focused specifically on the rapidly evolving science of RAS-addicted cancers. Equipping clinical staff with the latest peer-reviewed pharmacological data ensures the highest standards of safety during the administration of complex experimental agents. A highly educated oncology workforce serves as the ultimate institutional defense against preventable clinical complications and costly medical malpractice litigation.
Ultimately, successfully integrating revolutionary pharmaceutical assets requires a fundamental transformation of traditional healthcare operational and financial management paradigms. By decisively implementing these strategic systemic solutions, visionary medical organizations can simultaneously achieve unprecedented clinical outcomes and dominant market share expansion. The future of profitable oncology care demands a relentless commitment to data-driven precision, administrative efficiency, and unwavering patient-centric clinical excellence.
Strategic Prevention Strategies for Future Oncology Portfolios
Proactive healthcare systems must immediately prioritize the widespread implementation of multi-cancer early detection screenings to fundamentally alter long-term oncology demographics. Identifying pancreatic malignancies during their absolute earliest localized stages drastically reduces the systemic reliance upon exorbitantly expensive late-stage salvage therapies. By shifting the clinical focus toward aggressive early diagnostic interventions, medical institutions can systematically prevent the devastating financial burdens associated with advanced metastatic disease.
Pharmaceutical manufacturers must intentionally diversify their internal research pipelines to prevent catastrophic corporate vulnerabilities stemming from singular drug class failures. Over-investing exclusively in RAS inhibitors creates a highly precarious financial situation if unforeseen biological resistance mechanisms suddenly render the entire therapeutic category obsolete. Strategic corporate resilience requires the simultaneous development of diverse immunological, targeted, and radiopharmaceutical assets to ensure continuous long-term corporate revenue generation.
Healthcare organizations must establish extremely stringent internal conflict-of-interest policies regarding the rapid clinical adoption of heavily marketed experimental pharmaceuticals. Independent clinical review committees must rigorously evaluate all novel therapeutics using strictly objective, peer-reviewed data completely devoid of aggressive manufacturer influence. This vital administrative firewall prevents the dangerous institutional over-utilization of expensive unproven medications, thereby protecting both vulnerable patients and fragile hospital budgets.
Regulatory agencies must proactively modernize their existing clinical trial approval frameworks to demand significantly higher standards of diverse demographic representation. Historically marginalized populations must be proportionally included within all Phase 3 investigations to ensure that resulting efficacy data universally applies to the general public. Preventing future systemic health disparities requires the uncompromising enforcement of equitable clinical research protocols at the absolute highest levels of the federal government.
Health systems must actively construct robust centralized biometric data repositories to continuously track the longitudinal real-world performance of newly approved oncology agents. These massive proprietary databases allow clinical analysts to quickly identify hidden patterns of delayed systemic toxicity that completely evaded initial regulatory scrutiny. Leveraging localized big data analytics empowers medical directors to proactively revoke institutional formulary approvals before widespread catastrophic patient harm occurs.
Academic medical centers must heavily incentivize foundational scientific research focusing specifically on the complex evolutionary mechanisms of secondary tumor resistance. Understanding exactly how malignant cells successfully bypass molecular glue therapies is absolutely critical for the preemptive development of next-generation combination treatment regimens. By aggressively funding basic biochemical research, visionary institutions can permanently stay one step ahead of highly adaptable and remarkably resilient oncological mutations.
Hospital procurement divisions must consistently maintain diverse supply chain networks to prevent catastrophic therapeutic interruptions during unforeseen global pharmaceutical manufacturing crises. Relying upon a singular exclusive distributor for critical life-saving oncology medications introduces an unacceptable level of operational risk for major healthcare enterprises. Strategic vendor diversification guarantees continuous patient access to essential chemical interventions, thereby preventing tragic clinical regressions directly caused by systemic logistical failures.
Healthcare policy advocates must aggressively lobby federal legislators to enact sweeping statutory reforms targeting predatory pharmaceutical pricing models. Unregulated exponential increases in the baseline cost of essential oncology medications directly threaten the fundamental macroeconomic stability of the entire national healthcare system. Implementing strict federal price-capping legislation represents the only viable long-term prevention strategy against the imminent collapse of accessible American medical care.
Medical institutions must proactively develop highly integrated palliative care programs that operate concurrently alongside aggressive precision oncology treatment protocols. Introducing specialized supportive care services immediately upon initial diagnosis drastically improves overall patient quality of life while simultaneously preventing costly unnecessary emergency room admissions. This holistic approach to comprehensive cancer management ensures that aggressive medical interventions never eclipse the fundamental humanistic elements of compassionate clinical care.
Corporate healthcare executives must absolutely demand total financial transparency from pharmaceutical manufacturers regarding their internal research and development cost structures. Understanding the true underlying economic drivers of massive specialty drug price tags empowers hospital negotiators to demand fairer institutional purchasing contracts. Preventing future financial exploitation requires the uncompromising systemic dismantling of the historically opaque and highly secretive global pharmaceutical pricing apparatus.
True prevention within the complex oncology sector requires a relentless organizational commitment to proactive strategic foresight and rigorous systemic accountability. By decisively anticipating future clinical bottlenecks and aggressive financial risks, elite healthcare systems can continuously provide unparalleled medical care without sacrificing institutional solvency. The ultimate victory against aggressive malignancies demands an exceptionally synchronized approach uniting groundbreaking scientific innovation with impenetrable operational resilience.
Carethix Key Takeaways on Precision Oncology Integration
- Strategic alliances with AI firms specializing in predictive diagnostics are essential to accelerate the discovery of new molecular vulnerabilities and ensure clinical superiority.
- The success of the daraxonrasib phase three trial has redefined economic valuation models, signaling explosive growth for biopharmaceutical firms focused on complex molecular glues.
- Pharmaceutical manufacturers must modernize patient support frameworks and financial assistance programs to navigate insurance complexities and prevent patient medication non-adherence.
- Healthcare executives are advised to restructure oncology budgets to accommodate revolutionary agents like daraxonrasib, which is now a baseline requirement for modern clinical accreditation.
- Institutions should embrace value-based contracting models to mitigate financial risks by linking pharmaceutical compensation to verifiable clinical outcomes.
- Expanding internal molecular tumor board capabilities is essential for optimizing the clinical deployment of multi-selective RAS inhibitors and preventing wasteful pharmaceutical expenditures.
- Investing in advanced liquid biopsy technologies offers a cost-effective mechanism for continuous monitoring of efficacy and early detection of drug resistance.
- Proactive healthcare systems must prioritize the widespread implementation of multi-cancer early detection screenings to reduce reliance on expensive late-stage salvage therapies.
- Regulatory agencies need to modernize clinical trial approval frameworks to demand higher standards of diverse demographic representation and prevent future systemic health disparities.
FAQs:
How will daraxonrasib’s 13.2-month survival rate impact pancreatic cancer treatment costs in 2026?
Daraxonrasib’s survival breakthrough may improve outcomes, but healthcare systems that ignore genomic infrastructure, payer resistance, and oncology budget restructuring could face severe long-term financial instability.
Why are FDA fast-track pancreatic cancer drugs creating major healthcare reimbursement risks?
Fast-track oncology approvals accelerate patient access, yet hospitals without strong prior authorization, pharmacovigilance, and value-based contracting systems risk massive reimbursement losses and operational disruption.
Can precision oncology therapies like daraxonrasib worsen healthcare inequality and patient access gaps?
Precision oncology can dramatically improve survival, but underfunded hospitals and uninsured patients may remain excluded if genomic testing access and financial assistance programs are not rapidly expanded.
What are the biggest financial risks of integrating RAS inhibitor therapies into hospital oncology programs?
Hospitals aggressively deploying expensive RAS inhibitors without molecular tumor boards, AI-driven pharmacy logistics, and resistance monitoring strategies could trigger unsustainable oncology cost escalation.
Will pancreatic cancer drug resistance reduce the long-term effectiveness of daraxonrasib treatment?
Daraxonrasib shows major clinical promise, but healthcare leaders who underestimate secondary tumor resistance and overproject perpetual efficacy may dangerously miscalculate future oncology profitability and patient outcomes.

