
GLP-1s cutting metastasis risk by 38–50% highlights the need for Carethix-guided strategies to secure smarter oncology outcomes.
Real-world case study: ASCO 2026 TriNetX Analysis and Implications
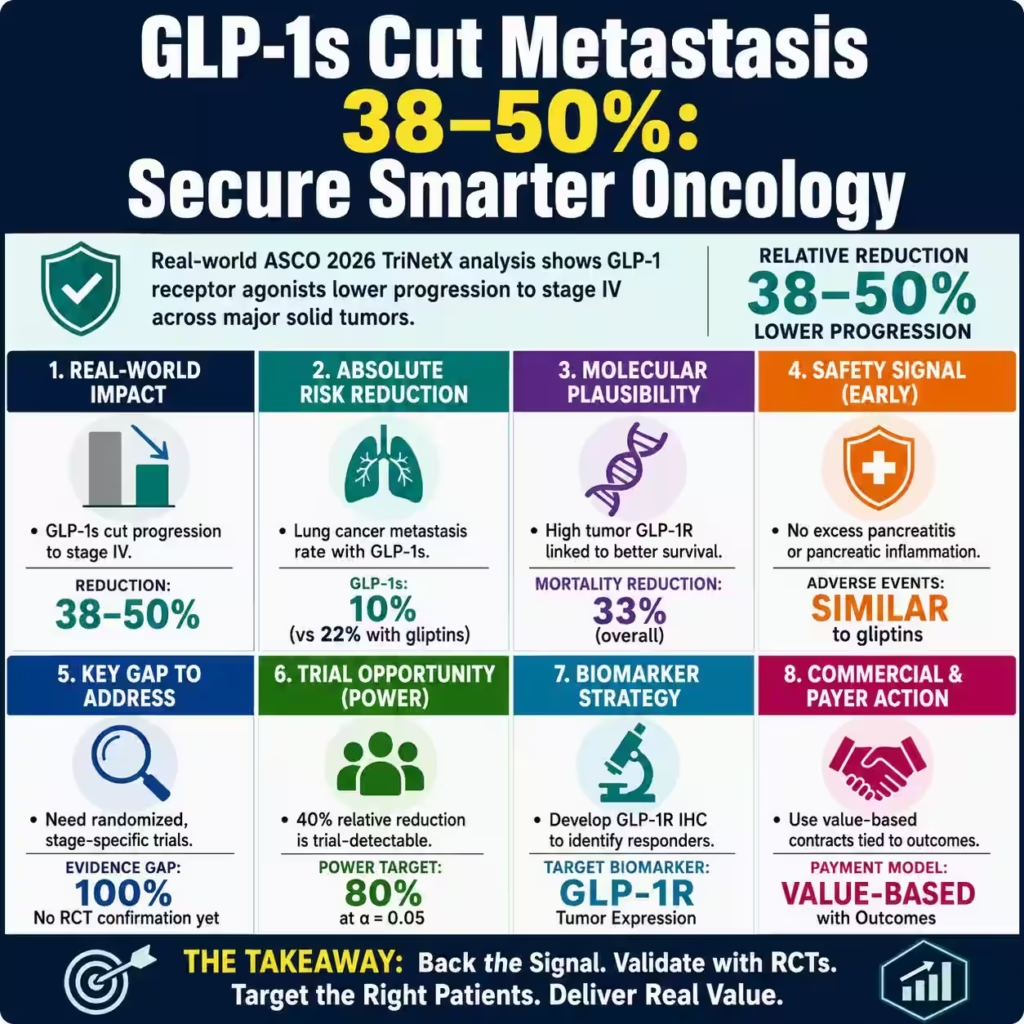
The TriNetX analysis of 12,112 patients presented at ASCO 2026 found that GLP-1 receptor agonist use was associated with a 38%–50% lower likelihood of progression to stage IV disease for lung, breast, colorectal, and liver cancers compared with DPP‑4 inhibitors (gliptins). These reductions translated into absolute metastasis rates of approximately 10% versus 22% for lung cancer, 10% versus 20% for breast cancer, 13% versus 22% for colorectal cancer, and 19% versus 28% for hepatocellular carcinoma in the GLP‑1 and gliptin cohorts respectively, highlighting clinically meaningful differences in progression risk. Carethix interprets these findings as an early yet robust real‑world signal that GLP‑1 signaling or GLP‑1 drug exposure may modulate tumor biology in select obesity‑related solid tumors, and this article outlines operational, clinical, and payer strategies to translate the signal into evidence‑based action while controlling safety and reimbursement risk.
The study’s cohort composition and data sources raise context‑specific considerations for external validity and deployment strategies. The sample included balanced exposure groups (roughly half GLP‑1 and half gliptin users) and diverse demographics — about 55–60% White, 20–25% Black or African American, and 10–15% Asian — which supports broad applicability but still requires subgroup validation for precision deployment. Complementary genomics analysis using The Cancer Genome Atlas data showed that high tumor GLP‑1R expression correlated with a 33% lower overall mortality, and a 45% lower mortality in breast cancer specifically, providing molecular plausibility to the real‑world clinical signal and a route for biomarker‑driven strategies.
High‑authority analysis: the design, magnitude, and limitations of the TriNetX signal
The magnitude of effect (38%–50% relative reduction in progression for four tumor types) exceeds typical real‑world effect sizes for off‑label pharmacologic impacts. Robust confounding control and sensitivity checks are essential before changing guidelines or reimbursement. TriNetX observational designs can adjust for measured confounders but remain susceptible to residual confounding (indication bias, unmeasured comorbidity, differential surveillance), therefore Carethix recommends prospective validation through randomized trials and registries to quantify absolute risk reduction and number needed to treat for each indication. The convergence of real‑world outcome differences and tumor GLP‑1R expression associating with survival strengthens causal inference but does not replace mechanistic and randomized confirmation; companies, payers, and oncology providers must therefore adopt an evidence‑graded, risk‑managed approach.
Carethix critique: risks, gaps, and industry implications
Carethix identifies three immediate gaps that constrain clinical translation: potential confounding in observational data, incomplete safety signal resolution for pancreas and GI inflammation, and the absence of randomized, stage‑specific efficacy data to support guideline changes. Although the ASCO report noted similar adverse event rates between GLP‑1 and gliptin groups and no excess pancreatitis or pancreatic inflammation in the GLP‑1 group, long‑term surveillance and structured safety endpoints are lacking to exclude rare but serious events. This is material for payers and hospital risk committees. From a health‑system perspective, rapid adoption without RCT validation risks misaligned formulary decisions and potential downstream costs if small absolute benefits prove inconsistent across subgroups or if off‑target harms appear in larger populations.
Carethix assessment of operational and equity risks for B2B stakeholders:
Real‑world databases like TriNetX may underrepresent certain care settings (e.g., community oncology clinics, underinsured populations), which could bias observed effectiveness and limit equitable deployment; 55–60% White and 20–25% Black representation in the dataset does not guarantee representative treatment access or outcomes across payer types. Pharmaceutical manufacturers and health systems must therefore avoid blanket messaging and instead pursue targeted pilot programs and value‑based contracting that tie reimbursement to prospective outcomes and safety monitoring. Finally, absent regulatory labeling for cancer progression indications, off‑label use may create medico‑legal and reimbursement friction unless supported by institutional protocols and documented consenting procedures.
Solutions: clinical, operational, and commercial pathways
Evidence generation and study design: Sponsor and academic stakeholders should initiate pragmatic randomized controlled trials in stage I–III patients with each implicated tumor type, using metastasis‑free survival and overall survival as co‑primary endpoints, and stratifying by GLP‑1R tumor expression. TriNetX effect sizes (38%–50% relative reduction) enable power calculations: for a baseline metastasis rate of ~22% (gliptin arm example, lung), a trial detecting a 40% relative reduction would require modest sample sizes per arm to achieve 80% power at alpha 0.05, facilitating feasible RCT design. Parallel prospective registries and propensity‑score matched emulations should run while RCTs proceed to supply early payer evidence and safety data.
Biomarker and companion diagnostics: Prioritize development of validated GLP‑1R immunohistochemistry assays and standardized thresholds to identify patients more likely to benefit, leveraging the TCGA signal (33% lower mortality with high GLP‑1R) as an evidence base. Diagnostic firms should pursue analytical and clinical validation plans with regulatory engagement to enable lab‑developed test deployment in integrated health systems, supporting precision prescribing and value‑based negotiations. Payers can negotiate coverage for diagnostic testing contingent on participation in registries that collect outcomes and safety endpoints.
Safety surveillance and stewardship: Implement structured pharmacovigilance with active monitoring for GI and pancreatic adverse events, linking EHR alerts to oncology safety committees and creating explicit stopping rules. Health systems should adopt prescribing pathways that require shared decision‑making documentation, baseline risk assessment for pancreatitis and pancreatic neoplasia, and scheduled imaging or biomarker follow‑up intervals to detect early progression or adverse events. Manufacturers should fund independent safety registries and support data harmonization across EHR systems to accelerate signal detection.
Payer and contracting strategies: Develop outcomes‑based agreements that tie a portion of GLP‑1 reimbursement to metastasis‑free survival outcomes or real‑world progression metrics captured in registries; given the potential for meaningful relative risk reductions observed, such agreements can align incentives while limiting short‑term budget impact. Include performance guarantees that account for diagnostic stratification (GLP‑1R positive vs negative) to optimize cost‑effectiveness and reduce heterogeneity of treatment effect. Use interim registry data to refine value assumptions and scale reimbursement pathways.
Prevention: steps to avoid future evidence and safety failures
Standardize data and endpoints: Harmonize outcome definitions (progression to stage IV, metastasis‑free survival) and covariates across real‑world datasets to reduce misclassification and allow reliable cross‑database meta‑analytics. Carethix recommends an industry working group to publish core outcome sets and minimum data standards for GLP‑1 oncology research within 6 months. This prevents variable definitions from producing spurious or non‑replicable signals that can mislead policy and clinical practice.
Pre‑specify confounder controls and sensitivity analyses: Registries and observational analyses must pre‑register covariates, instrumental variable analyses, and negative‑control outcomes to transparently bound causal claims. This reduces the risk of premature guideline shifts based on biased estimates. Data sharing agreements should enable independent replication by academic groups to validate original findings. Such methodological rigor prevents regulatory or payer reversals that harm credibility and patient trust.
Phased clinical adoption with governance: Health systems should put GLP‑1 oncology use into a controlled roll‑out with institutional review board oversight, predefined inclusion criteria, and mandatory registry enrollment; this limits off‑label diffusion and ensures coordinated monitoring. Embed equity safeguards to ensure underrepresented groups are included in trials and registries to avoid widening care disparities. This governance model reduces legal and fiscal exposure while enabling timely access for patients who may benefit.
Transparent communication and education: Develop standardized clinician and patient materials that clearly describe the level of evidence, known benefits, potential risks, and alternatives, and update them as trial and registry data mature. Manufacturers and clinical leaders should avoid overstated claims and instead present conditional, evidence‑graded guidance to maintain professional trust. Transparent communication prevents inappropriate demand shifts and supports ethical, evidence‑based care.
Carethix Key Takeaway
Carethix views the TriNetX ASCO 2026 signal — a 38%–50% relative reduction in metastatic progression for four obesity‑related cancers and a 33% lower mortality with high tumor GLP‑1R expression — as a high‑priority, high‑opportunity finding that requires immediate, disciplined action across trials, diagnostics, safety monitoring, and payer contracting. Implement phased, biomarker‑guided pilots, fund pragmatic RCTs, and align payers through outcomes‑based agreements while maintaining rigorous pharmacovigilance and standardized data practices to translate the signal into responsible clinical benefit. Acting now with methodical evidence generation and governance will protect patients, limit financial risk, and position your organization as a leader in integrating metabolic therapeutics into oncology care.
FAQs:
1. Can GLP-1 Drugs Reduce Metastatic Cancer Progression by 38%–50% in Lung, Breast, and Colorectal Cancer?
The ASCO 2026 TriNetX analysis involving 12,112 patients reported a striking 38%–50% lower progression to stage IV disease among GLP-1 receptor agonist users compared with DPP-4 inhibitor cohorts, including lung cancer metastasis rates falling from 22% to 10% and breast cancer progression declining from 20% to 10%. However, the oncology industry should avoid premature commercialization because observational databases remain vulnerable to indication bias, surveillance bias, and residual confounding that can exaggerate apparent therapeutic impact. Healthcare systems pursuing GLP-1 oncology integration should prioritize randomized controlled trials, biomarker-driven patient selection, and outcomes-based reimbursement contracts before scaling high-cost adoption pathways.
2. Why Are GLP-1 Oncology Trials Becoming a High-Value Investment Opportunity After ASCO 2026?
The reported 40% relative reduction in metastatic progression across obesity-related cancers creates a potentially multibillion-dollar oncology expansion opportunity for companies developing GLP-1 therapeutics, companion diagnostics, and precision oncology infrastructure. Yet the current evidence base lacks randomized stage-specific efficacy validation, making aggressive payer expansion and off-label prescribing financially risky if future trials fail to replicate real-world outcomes. Pharmaceutical firms that move first with pragmatic RCTs, GLP-1R biomarker assays, and value-based contracting frameworks will likely dominate payer negotiations and oncology formulary positioning over the next 3–5 years.
3. Are GLP-1 Receptor Agonists Safe for Cancer Patients Despite Pancreatitis and GI Inflammation Concerns?
Although the ASCO 2026 dataset found no measurable increase in pancreatitis or pancreatic inflammation among GLP-1 users versus gliptin users, the absence of long-term pharmacovigilance data remains a major concern for oncology safety committees and regulators. The cancer care industry has repeatedly underestimated delayed safety liabilities in rapidly adopted therapies, and even rare adverse events could trigger reimbursement reversals or litigation exposure if millions of oncology patients receive expanded GLP-1 access. Hospitals and pharmaceutical manufacturers should therefore implement structured adverse-event monitoring, mandatory registry participation, and standardized GI risk assessment protocols before integrating GLP-1 therapies into broader metastatic prevention strategies.
4. How Important Is GLP-1R Biomarker Testing After the 33% Lower Mortality Signal in Cancer Patients?
The complementary TCGA genomics analysis showing 33% lower overall mortality — including a 45% lower mortality rate in breast cancer patients with high tumor GLP-1R expression — significantly strengthens the precision oncology case for biomarker-guided treatment deployment. However, many healthcare organizations still lack standardized GLP-1R immunohistochemistry testing workflows, which could create inconsistent patient selection and inflated treatment costs if broad prescribing occurs without molecular stratification. Diagnostic firms that rapidly validate GLP-1R assays and align them with payer-supported registry programs may become critical infrastructure providers in the next generation of metabolic oncology care.
5. Will Outcomes-Based Contracts Become Essential for GLP-1 Cancer Treatment Reimbursement?
With metastatic progression reductions reaching as high as 50% in some tumor categories, payers are increasingly likely to demand outcomes-based reimbursement models tied to metastasis-free survival, registry evidence, and biomarker-confirmed patient response. The financial risk of unrestricted off-label oncology expansion is substantial because GLP-1 therapies already carry high annual treatment costs and uncertain long-term oncology efficacy durability. Insurers, hospital systems, and pharmaceutical manufacturers that fail to establish evidence-linked contracting structures could face major budget overruns, reimbursement disputes, and regulatory scrutiny as demand for GLP-1 cancer prevention strategies accelerates globally.

