
Lyme’s 22% surge exposes urgent gaps in care as Carethix outlines strategies to accelerate diagnosis, prevention, and treatment outcomes.
Deep Case Study: England’s 22% Lyme Disease Surge Exposes Critical Healthcare System Gaps
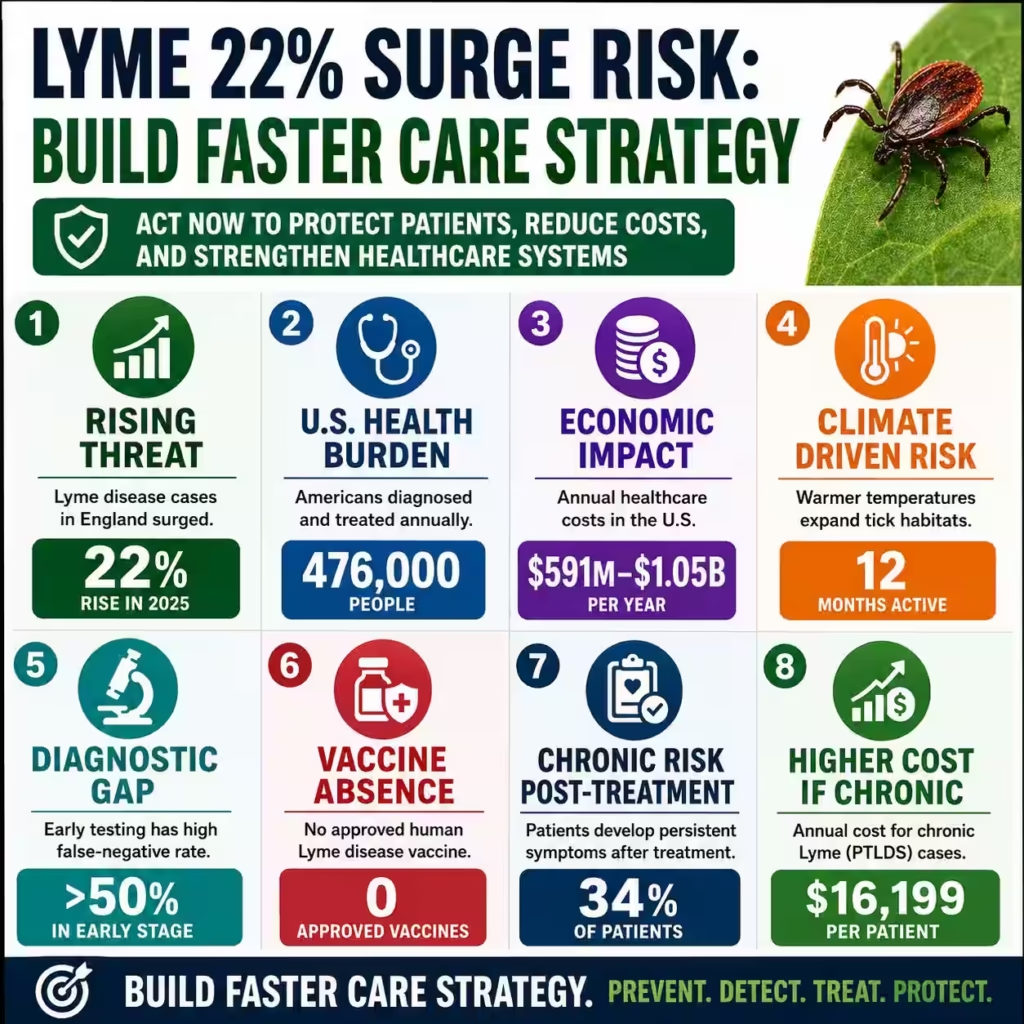
Cases of Lyme disease in England rose over 20% in one year. The UK Health Safety Agency confirmed 1,168 cases in 2025, up from 959 cases in 2024. This represents a 22% increase revealing serious gaps in public health surveillance. The disease comes from bacteria spread by ticks that feed on animal and human blood. Untreated Lyme disease can cause chronic joint pain, neurological problems, facial muscle paralysis, and heart complications.
Early symptoms look like the flu and may include a circular rash called a bullseye rash. This rash can appear up to three months after an infected tick bites someone. If left untreated, the disease can cause memory problems, concentration issues, and inflammation of the brain or spinal cord. Many patients do not get diagnosed quickly because early test results often come back negative. This delay in treatment leads to chronic illness in about 40% of cases.
The United States faces a similar problem with about 476,000 diagnosed annually. Annual healthcare costs for Lyme disease in the US range from $591 million to $1.05 billion. Patients with Lyme disease pay about $4,100 more in healthcare costs over six months compared to people without the disease. They also have 87% more outpatient visits and 71% more emergency visits a year after diagnosis. These numbers show that delayed diagnosis creates huge financial strain on healthcare systems.
Thirty-four percent of patients who receive treatment still develop persistent symptoms called Post-Treatment Lyme Disease Syndrome. These chronic patients face annual costs averaging $16,199, while early-stage disease costs only $1,300 per patient. The out-of-pocket cost for patients averages $1,200 per illness. Employers also lose money through reduced productivity and disability claims from workers with chronic Lyme disease. This burden will grow as climate change expands tick habitats northward.
Warmer temperatures are making ticks active for longer periods each year. Tick bites now happen year-round but peak in June during late spring. The UKHSA reports that Lyme disease remains England’s most common locally acquired vector-borne infection. Two probable cases of tick-borne encephalitis were also found in 2025 without international travel. This brings the total locally acquired human cases to six since the virus first appeared in the UK in 2019. Climate change, habitat loss, and growing deer populations all contribute to rising tick numbers.
Current diagnostic tests have poor sensitivity during early infection stages. False-negative rates exceed 50% in the first weeks after a tick bite. This is when antibiotic treatment works best to prevent chronic illness. Only 70 to 80% of patients develop the characteristic bullseye rash. The remaining 20 to 30% without this key warning sign. Most electronic health records do not have tools to guide treatment when clinical suspicion is high but lab tests are negative.
There is no approved human Lyme disease vaccine today. The last vaccine was withdrawn from the market in 2002 due to low demand and lawsuits. Pfizer and Valneva are testing a new vaccine called VLA15 in Phase 3 trials. Regulatory submissions are expected in 2026, but the vaccine may not launch until late 2027. This means patients will wait at least two years without effective primary prevention. Healthcare organizations must act now rather than wait for a vaccine that may not arrive on time.
Carethix Critique: Critical Gaps in Current Lyme Disease Management Create Unacceptable Patient and Financial Risk
Carethix identifies four major failures in current Lyme disease management. These failures expose healthcare systems to serious clinical, financial, and reputational risk. Patients remain vulnerable to preventable chronic disability because of these gaps. The first failure is the complete absence of an approved human Lyme disease vaccine. This preventive medicine gap has persisted for decades despite 476,000 annual US cases. The disease costs nearly $1 billion each year in healthcare expenses.
The pharmaceutical industry has delayed vaccine deployment for too long. Pfizer and Valneva’s VLA15 candidate remains in Phase 3 trials. Regulatory submissions are expected in 2026 with a potential launch in late 2027. Patients will remain without effective primary prevention for at least two years. This delay contradicts basic public health principles for vaccine-preventable diseases. Lyme disease receives less than 2 percent of public funding allocated to West Nile virus. It receives only 0.2 percent of HIV/AIDS funding despite having far more cases than both diseases combined.
The second failure involves poor diagnostic testing protocols. Current two-tier serological testing has poor sensitivity during early localized disease. False-negative rates exceed 50 percent within the first weeks of infection. This is when antibiotic treatment is most effective at preventing chronic disease. Diagnostic failure forces clinicians to make treatment decisions based on clinical judgment alone. This creates practice variation that delays treatment for about 40 percent of patients. Other patients receive unnecessary antibiotic exposure due to false alarms.
The characteristic bullseye rash appears in only 70 to 80 percent of cases. This means 20 to 30 percent of patients without this key diagnostic marker. Most electronic health records lack structured decision support tools. These tools should guide appropriate empiric treatment when clinical suspicion remains high. Without them, clinicians miss opportunities to treat early and prevent chronic complications. The result is more patients developing long-term disability from preventable disease progression.
The third failure is the lack of standardized post-treatment monitoring protocols. Thirty-four percent of patients develop persistent symptoms after completing antibiotic treatment. These patients have Post-Treatment Lyme Disease Syndrome but receive fragmented care. Insurance coverage for extended care remains inconsistent across different payers. Many insurers deny coverage for treatments beyond the initial antibiotic course. This happens despite evidence showing chronic patients need average annual costs of $16,199. Early disease patients only need $1,300 in annual care costs.
This coverage gap forces patients into out-of-pocket spending averaging $1,200 per illness. Employers absorb productivity losses from chronic disability affecting workplace attendance. Workers with disseminated Lyme disease generate workers’ compensation claims averaging $12,000 each. The fourth failure involves inadequate public health messaging around tick bite prevention. Guidance remains inconsistent across different health agencies and regions. There are no mandatory employer requirements for outdoor workers despite high exposure risks.
Occupational exposure risks exceed general population levels by 3 to 5 times in high-prevalence regions. The UKHSA recommends avoiding tick bites and using tick removal devices. Yet pharmacy sales data shows tick removal tools remain niche products. They are not standard first-aid supplies in most homes or workplaces. Workplace safety regulations fail to mandate tick prevention training for landscaping workers. Forestry, construction, and agricultural workers also lack required protection protocols.
This regulatory gap leaves employers exposed to workers’ compensation claims. Employers also face OSHA citations for failing to protect outdoor workers. Patients receive conflicting guidance about proper tick removal techniques. Many people use incorrect methods that squeeze the tick body. This increases bacterial transmission risk by forcing infected saliva into the bloodstream. Healthcare systems must fix these gaps before costs and disability rates climb higher.
Comprehensive Solutions: Integrated Clinical, Technological, and Operational Strategies to Address Lyme Disease Burden
Healthcare organizations must implement a multi-layered solution framework. This framework should address diagnostic accuracy, preventive care delivery, patient education, and operational efficiency. The goal is to reduce Lyme disease incidence and improve early treatment rates. It also aims to minimize chronic disease complications that drive up costs. The first critical solution involves deploying artificial intelligence-powered clinical decision support systems. These systems should integrate into electronic health records at all practice locations.
The AI system should trigger Lyme disease evaluation protocols when patients present with flu-like symptoms. This should happen during tick season in endemic areas. The system should include structured risk assessment fields capturing outdoor exposure history. It should also capture occupational hazards and geographic location data. These AI systems should use machine learning algorithms trained on confirmed case data. Algorithms calculate individualized probability scores for each patient.
The system should prompt clinicians to consider empiric antibiotic treatment when clinical suspicion exceeds 15 percent. This should happen even when initial serology tests are negative. Doing so reduces treatment delays that drive chronic disease progression. Early treatment within 72 hours of tick bite has antibiotic efficacy exceeding 90 percent. Delayed treatment drops efficacy significantly and increases chronic disease risk by 40 percent.
The second essential solution requires healthcare payers and employers to establish preventive care benefit packages. These packages should cover tick removal device distribution at no cost to patients. They should also cover comprehensive tick bite education programs. Post-exposure prophylaxis protocols should be available for high-risk patients. Insurance plans should provide $15 to $25 tick removal tools through pharmacy benefit managers. These tools should have no copay, similar to glucose monitoring supplies for diabetes.
Employers should mandate annual tick prevention training for all outdoor workers. They should distribute protective clothing including permethrin-treated uniforms. These treated uniforms reduce tick attachment by 85 percent. Healthcare systems should partner with occupational health providers to create workplace-specific prevention protocols. These protocols should include pre-shift tick inspection procedures before work begins. Workers should remove outdoor clothing before entering work facilities to prevent bringing ticks inside.
Same-day medical evaluation should be required for documented tick bites. This ensures treatment within 72 hours when antibiotic efficacy exceeds 90 percent. Doing so reduces progression to disseminated disease significantly. The third solution requires healthcare organizations to invest in next-generation diagnostic development. Point-of-care molecular testing platforms should deliver results within 30 minutes. These tests should have sensitivity exceeding 95 percent during early infection stages.
Rapid diagnostic tests should use polymerase chain reaction technology. This technology detects Borrelia burgdorferi DNA directly from skin biopsy samples or blood. It eliminates the window period limitations of serological testing. Serological testing requires 2 to 6 weeks for antibody development. Point-of-care testing works during this critical early window when treatment matters most. Early adoption of these technologies should begin at academic medical centers.
Value-based reimbursement negotiations with payers should demonstrate cost savings. Savings come from reduced hospitalizations and decreased chronic disease complications. Improved productivity also contributes to overall cost savings. Health economic models show $4.50 return on investment for every dollar spent. This return comes through avoided chronic care costs averaging $14,899 per patient. The fourth solution involves pharmaceutical partnerships to accelerate vaccine development.
Public-private funding models should de-risk investment while ensuring affordable pricing. Healthcare systems should establish early access programs for clinical trial enrollment. These programs create patient registries tracking vaccine efficacy in real-world populations. The registries generate post-market surveillance data required for regulatory approval. Programs should prioritize high-risk populations including outdoor workers and children ages 5 and older. Patients with recurrent tick exposures should also receive priority access.
Healthcare organizations should negotiate preferred network status upon vaccine approval. Value-based pricing contracts should guarantee cost-per-case-prevented thresholds below $500. This compares favorably to average chronic disease costs exceeding $16,000 per patient. Pfizer and Valneva target launch in the second half of 2027. Healthcare systems should prepare now through provider education programs. Storage and handling infrastructure upgrades should happen before vaccine arrival. Insurance formulary placement strategies should ensure immediate access upon FDA approval.
The fifth solution requires integrated One Health surveillance systems. These systems connect human clinical data with veterinary diagnostic results. Environmental tick monitoring data should also feed into the system. This creates predictive risk mapping identifying emerging hotspots before human cases surge. Geographic information systems should map tick density and host animal populations. Climate variables and human case data should also be included in mapping.
Risk scores should update weekly to enable proactive public health interventions. Interventions include targeted media campaigns and mobile testing clinics. Preemptive provider education should occur in high-risk zip codes before cases appear. Health systems should partner with universities and state health departments. Data sharing through standardized APIs creates national surveillance networks. These networks detect regional transmission patterns and enable rapid response to emerging threats. Response should happen before outbreaks exceed 1,000 cases annually like England’s current situation.
Prevention Steps: Proactive Measures to Mitigate Future Lyme Disease Risks Before They Become Costly Crises
Healthcare executives must implement immediate prevention protocols starting with staff education. Comprehensive programs should train all clinical personnel on Lyme disease recognition. Training should cover appropriate testing protocols and evidence-based treatment guidelines. This ensures consistent care delivery across all practice settings. Programs should include mandatory annual training modules covering updated CDC guidelines.
Training should cover recognition of atypical presentations including patients without bullseye rash. Proper tick removal techniques using fine-tipped tweezers should be demonstrated. Tweezers should grasp the tick close to skin without squeezing the body. Documentation requirements should capture exposure history and removal timing. Clinical decision rationale should be documented to support quality improvement initiatives. This documentation also helps defend against malpractice claims arising from delayed diagnosis.
Training completion should be tracked through learning management systems. Mandatory competency assessments require 90 percent passing scores before credential renewal. This ensures all providers maintain current knowledge as guidelines evolve. Second, healthcare organizations must establish workplace environmental control programs. These programs serve facilities with outdoor exposures including landscaping crews and maintenance staff. Field service technicians also need protection through these programs.
Tick habitat reduction strategies should be implemented around building perimeters. Vegetation management should create 9-foot wide wood chip or gravel barriers. These barriers between lawns and woodlands reduce tick populations 70 to 80 percent. Weekly tick inspections should occur during peak season from May through September. Drag cloth sampling methods identify hotspot areas requiring targeted acaricide application. Results should be documented and shared with occupational health teams monthly.
Exposure risk assessments should update monthly based on inspection results. Facilities should provide permethrin-treated work clothing replacing employee-provided attire. Tick removal kits should be distributed to all outdoor workers regularly. Mandatory post-exposure medical evaluation within 24 hours of documented tick bites should be required. This creates institutional accountability preventing expensive workers’ compensation claims. Workers with disseminated Lyme disease generate claims averaging $12,000 each.
Third, healthcare systems should develop patient-facing digital health tools. Mobile applications should provide real-time tick risk forecasts based on local weather data. Interactive tick identification guides should distinguish disease-carrying species from harmless varieties. Automated reminder systems should prompt post-bite medical evaluation when users log tick encounters. These applications should integrate with wearable devices tracking outdoor activity duration. Location data generates personalized risk assessments for each user.
Push notifications should send alerts when users enter high-risk areas during peak tick activity. Health systems should promote these tools through patient portals and email campaigns. Social media channels should reach 500,000+ members annually. Engagement metrics should track download rates and active users. Reported tick bites should be monitored to measure program effectiveness. Continuous improvement of prevention messaging follows from data analysis.
Resource allocation decisions follow from engagement and outcome metrics. Fourth, healthcare organizations must establish community partnerships with schools and parks departments. Recreational facilities should also join these partnerships to create tick-safe zones. Landscape modifications should include wood chip pathways replacing dirt trails. Regular leaf litter removal reduces tick habitat around recreational areas. Deer exclusion fencing reduces tick populations by 90 percent in targeted areas.
Educational booths at community events should operate during spring and summer months. Tick removal tools should be distributed with protective clothing and educational materials. These events should reach 10,000+ community members annually. Follow-up surveys should measure knowledge improvement and behavioral changes. Increased tick check frequency should result from education programs. Proper removal technique adoption should increase after hands-on demonstrations.
Community-level outcomes should track emergency department visits for tick bites. Lyme disease incidence in target zip codes should decrease over time. Patient satisfaction scores related to preventive care access should improve. These metrics demonstrate return on investment through avoided healthcare costs. Enhanced community health reputation also benefits the health system financially. Fifth, healthcare executives must establish board-level oversight committees monitoring Lyme disease metrics.
Case counts by practice location should be tracked monthly. Time-to-diagnosis intervals should be measured against benchmarks. Chronic disease progression rates should be compared to national averages. Total cost per case should be tracked and compared to benchmarks regularly. These metrics create accountability structures ensuring Prevention strategies receive sustained executive attention. Dedicated budget allocation should exceed $500,000 annually for mid-sized health systems.
Cross-functional teams should coordinate clinical operations, IT, finance, and community outreach. Fragmented efforts fail against a threat expanding through climate change. Habitat encroachment and inadequate public awareness also drive case increases. Committees should meet quarterly reviewing dashboards displaying key performance indicators. Color-coded alert systems should trigger intervention when metrics exceed thresholds. Diagnosis delays exceeding 14 days should trigger immediate review. Chronic disease rates surpassing 30 percent should also trigger intervention.
Committee members should include clinical leaders and quality improvement specialists. Finance executives and patient advocates should also serve on committees. This ensures balanced perspectives addressing clinical effectiveness and financial sustainability. Patient experience should also be considered in all decisions. Annual public reporting should demonstrate organizational commitment to combating this growing infectious disease threat. Healthcare systems across North America and Europe face this challenge together.
Carethix Key Takeaway
Carethix asserts that healthcare organizations ignoring Lyme disease prevention will face escalating financial losses. The 22 percent year-over-year increase in England predicts a similar US trajectory. Case counts could approach 600,000 annual cases within five years. This would multiply current $1 billion annual costs to $2 billion annually. Chronic disease complications would affect 200,000+ patients each year.
No approved vaccine until 2027 requires immediate action. Healthcare systems must invest in diagnostic innovation now. Workplace prevention programs should launch immediately rather than waiting. Integrated One Health surveillance should be deployed before case counts surge further. Waiting for pharmaceutical solutions transfers unacceptable risk to patients. Healthcare systems absorb mounting costs through increased utilization and disability claims. Malpractice exposure also increases with each delayed diagnosis.
Healthcare executives must treat Lyme disease as a strategic priority requiring board-level oversight. Dedicated budget allocation should exceed $500,000 annually for mid-sized health systems. Cross-functional teams should coordinate clinical operations, IT, finance, and community outreach. Fragmented efforts fail against a threat expanding through climate change and habitat encroachment. Inadequate public awareness also drives case increases across all regions.
Your organization’s decision to invest now determines your future position. Comprehensive Prevention infrastructure creates industry leadership in population health management. Delayed action makes your organization a cautionary example of reactive crisis management. Reactive management costs 10 times more than proactive prevention annually. Patient trust suffers when preventable chronic disability occurs due to system failures. Regulatory compliance standing also damages when prevention standards are not met. Act now to protect patients, employees, and your organization’s financial future.
FAQs:
1. Why Is Lyme Disease Rising 22% in England, And What Does It Mean for Healthcare Costs in 2026?
England’s confirmed Lyme disease cases surged from 959 in 2024 to 1,168 in 2025, while the US already records nearly 476,000 annual diagnoses, exposing how climate change, expanding tick habitats, and weak preventive infrastructure are overwhelming healthcare systems. The larger problem is that most healthcare organizations still treat Lyme disease as a seasonal nuisance instead of a long-term population health and occupational risk management crisis. Without AI-driven surveillance, rapid molecular diagnostics, and mandatory outdoor worker prevention programs, healthcare costs could exceed $2 billion annually within five years as chronic Lyme complications accelerate disability claims and emergency utilization.
2. How Much Does Chronic Lyme Disease Cost Employers, Insurers, and Healthcare Systems?
Patients with Lyme disease generate nearly $4,100 more healthcare spending within six months compared to non-Lyme patients. Chronic Post-Treatment Lyme Disease Syndrome cases average $16,199 annually versus just $1,300 for early-stage treatment. The financial damage extends beyond hospitals because employers absorb productivity losses, absenteeism, workers’ compensation exposure, and long-term neurological disability claims that continue for years after delayed diagnosis. Healthcare executives ignoring early detection investment are effectively accepting a 10x higher downstream cost burden caused by outdated testing protocols and fragmented post-treatment monitoring systems.
3. Why Are Current Lyme Disease Diagnostic Tests Failing Nearly 50% of Early Cases?
Current two-tier serological Lyme disease testing can produce false-negative rates exceeding 50% during the first weeks of infection when antibiotics are most effective and chronic progression is still preventable. The dangerous gap is that 20% to 30% of patients never develop the classic bullseye rash, yet most electronic health record systems still lack structured AI-powered clinical decision support to guide empiric treatment decisions. Healthcare systems relying on outdated diagnostics are creating preventable neurological complications, heart inflammation, and chronic pain syndromes that later become expensive litigation, payer disputes, and reputation risks.
4. Can AI and Rapid Molecular Testing Reduce Lyme Disease Misdiagnosis and Chronic Illness?
AI-powered clinical decision support integrated with electronic health records could dramatically reduce delayed treatment by identifying high-risk patients based on geography, outdoor exposure, occupational history, and symptom patterns before laboratory confirmation arrives. Point-of-care molecular diagnostics delivering results within 30 minutes with sensitivity above 95% would eliminate the dangerous 2-to-6-week antibody window period responsible for thousands of preventable chronic cases annually. Healthcare organizations delaying adoption of predictive AI surveillance and rapid PCR testing are falling behind a disease trend that is becoming increasingly climate-driven, year-round, and operationally expensive.
5. Why Is Lyme Disease Becoming a Major Occupational Health and ESG Risk for Businesses?
Outdoor workers in landscaping, forestry, agriculture, and construction face Lyme disease exposure risks estimated to be 3 to 5 times higher than the general population, yet most employers still lack mandatory tick prevention policies and standardized response protocols. This creates a serious ESG, workforce safety, and regulatory liability issue because untreated Lyme disease can trigger chronic neurological symptoms, reduced productivity, and workers’ compensation claims averaging thousands of dollars per affected employee. Businesses that fail to implement preventive measures such as permethrin-treated uniforms, mandatory tick inspections, AI risk mapping, and same-day medical evaluation are exposing themselves to escalating operational and reputational damage as vector-borne diseases expand globally.

