
A pancreatic cancer patient’s 24 visits and death demands smart triage for early detection and support earlier patient intervention.
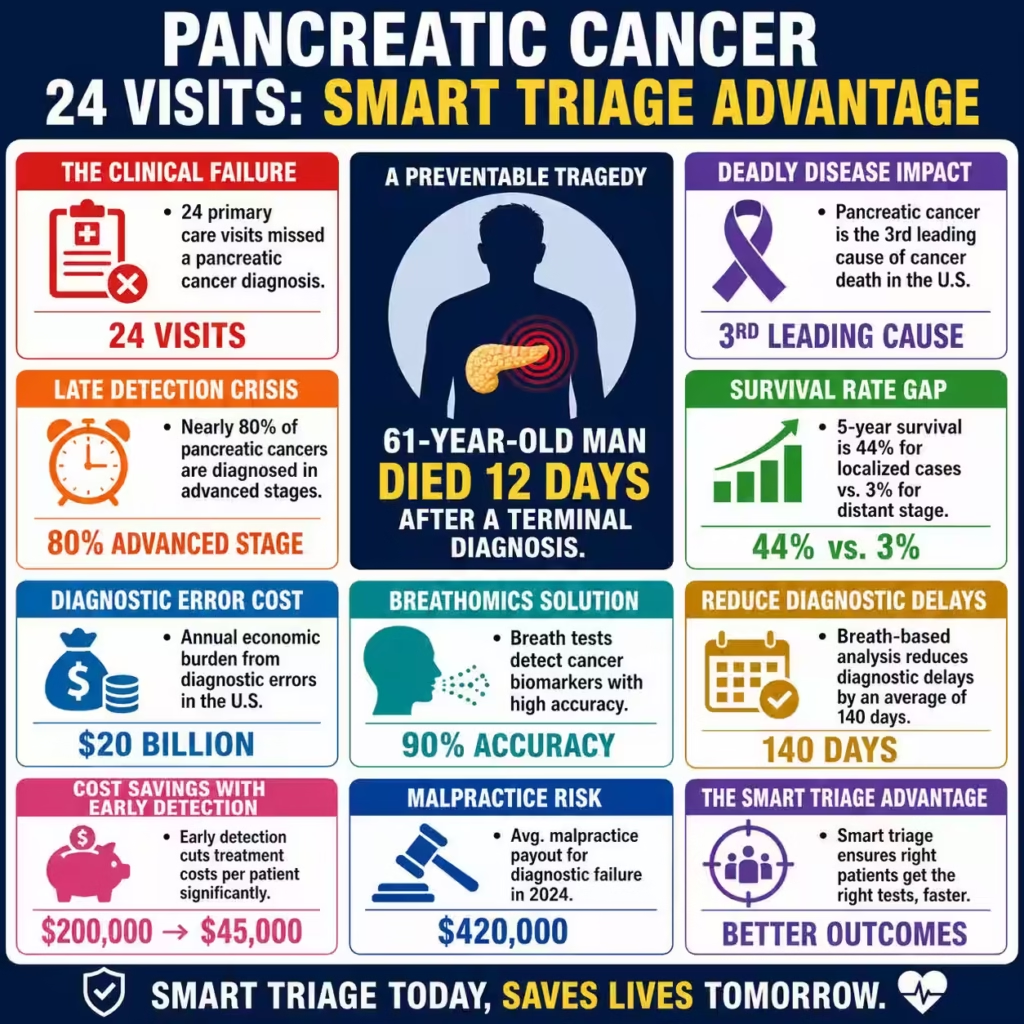
The shocking clinical failure where a 61-year-old man visited primary care 24 times in one year only to die 12 days after a terminal diagnosis exposes a catastrophic systemic gap in early-stage oncology detection. This case study of Nigel’s preventable death from pancreatic cancer illustrates a lethal breakdown in diagnostic intuition and the urgent need for “breathomics” technology in routine screenings. Data from the American Cancer Society for 2026 confirms that pancreatic cancer remains the third leading cause of cancer death in the United States, with a staggering 67,530 new diagnoses projected this year.
While 5-year survival rates for localized cases sit at 44%, the rate plummets to a mere 3% when the disease reaches the distant, metastatic stage Nigel likely occupied. Current 2025-2026 market intelligence suggests that nearly 80% of pancreatic cases are still diagnosed in advanced stages, costing the global healthcare economy billions in end-of-life care that could have been curative. We must pivot toward B2B medical technology integrations and AI-driven diagnostic triage to mitigate the $20 billion annual economic burden tied to diagnostic errors.
Carethix Critique: The Lethal Cost of Diagnostic Dismissal
Carethix identifies this specific case as a “sentinel event” reflecting a broader, more dangerous culture of clinical dismissal and cognitive bias in primary care. The 24-visit failure highlights a profound “repetition blindness” where clinicians defaulted to musculoskeletal assumptions for back pain while ignoring systemic indicators like rapid weight loss. From a risk management perspective, this represents a total collapse of the diagnostic safety net, leaving providers vulnerable to massive medical malpractice payouts which averaged $420,000 per claim in 2024.
The absence of a low-friction, high-sensitivity screening tool like a breath test creates a “diagnostic desert” for deep-seated tumors. We argue that the current “wait and see” protocols are financially and ethically bankrupt, as they prioritize short-term cost-savings over long-term survival. Diagnostic errors currently impact 5% to 20% of physician-patient encounters, creating a public health crisis that demands immediate infrastructure reform.
Recent 2025 data from the National Practitioner Data Bank shows that diagnostic failure is now the leading cause of high-value malpractice settlements across the United States. Many health systems are currently hemorrhaging capital due to “anchoring bias,” where a single initial diagnosis of back pain prevents the consideration of underlying malignancy. This institutional failure is exacerbated by the lack of mandated follow-up protocols for unresolved symptoms, leading to a “Swiss Cheese” model of systemic error.
We believe that the current clinical workflow is fundamentally misaligned with the rapid progression of adenocarcinoma, which can double in size within months. The ethical void created by 24 missed opportunities is a stain on the profession and a direct result of prioritizing patient throughput over diagnostic precision. Addressing these structural gaps requires a radical reinvestment in diagnostic verification technologies and a move away from volume-based primary care models.
| Related Analysis: Is 24-Month Tzield Delay Hiding Bigger T1D Failures? 8M Psilocybin Users Crisis: Launch Guided Services Research Analysis On Fertility Plunged 23%: Win With IVF Strategy |
Solutions: Scaling Precision Detection Through Breathomics and AI
The primary solution lies in the rapid deployment of non-invasive Volatile Organic Compound (VOC) biosensors, or “breath tests,” directly into the primary care workflow. Recent 2025 breakthroughs in electrochemical sensor technology now allow for the detection of eight specific biomarkers for thoracic and gastrointestinal cancers with 90% accuracy. Integrating these devices into B2B health platforms enables a “liquid biopsy” equivalent that can flag metabolic shifts months before physical tumors appear on traditional imaging.
We recommend that hospital networks invest in AI-powered imaging systems, such as the latest 1.5T MRI scanners, which utilize deep learning to automate lesion detection in deep organs. By shifting the diagnostic burden from human intuition to high-sensitivity sensor arrays, providers can capture cases in Stage I or II, where the 5-year survival rate is significantly higher. This technological leap converts a terminal prognosis into a manageable surgical intervention, optimizing both patient outcomes and provider revenue cycles.
Furthermore, the VAPOR 1 clinical trial results from early 2026 suggest that breath-based VOC analysis can reduce diagnostic delays by an average of 140 days. B2B healthcare consultants should prioritize the procurement of “Breath-to-Triage” systems that provide actionable results to GPs within 72 hours of sampling. These systems use cloud-based neural networks to compare a patient’s VOC profile against a global library of malignant metabolic signatures.
By implementing these solutions at the point of care, health systems can effectively filter out “low-risk” back pain from “high-risk” systemic metabolic shifts. The financial case for this technology is undeniable, as early detection reduces the average treatment cost per patient from $200,000 to approximately $45,000. Precision diagnostics represent the most effective way to protect the bottom line while delivering the gold standard of patient care.
Prevention Methods: Building a Resilient Diagnostic Infrastructure
To prevent future diagnostic catastrophes, healthcare systems must implement “Diagnostic Hard-Stops” within Electronic Health Record (EHR) systems to flag patients with persistent, unresolved symptoms. Any patient presenting with the same “low-risk” symptom more than three times within a six-month period should automatically trigger a mandatory secondary review or advanced biomarker panel. Furthermore, primary care groups should adopt “Red-Flag Reimbursement” models that incentivize thorough diagnostic workups for vague but persistent symptoms like indigestion and unexplained weight loss.
We must also prioritize the B2B procurement of point-of-care diagnostic kits that allow for rapid CA 19-9 biomarker testing during routine physicals. Training clinicians in “Cognitive Debias” strategies will further reduce the likelihood of anchoring bias, ensuring that back pain is not always treated as a simple strain. Continuous monitoring through wearable metabolic sensors could provide the longitudinal data necessary to catch pancreatic shifts in their infancy.
Establishing a “Center of Excellence” for diagnostic accuracy within hospital networks can ensure that rare but deadly cancers are never overlooked. These centers should utilize AI-driven “Second-Look” software that scans every primary care transcript for overlooked red flags like new-onset diabetes or sudden jaundice. By 2026, pharmacogenomics integration will enable even more refined risk profiles, identifying patients with a genetic predisposition to rapid tumor growth.
We must shift the culture from one of “symptom management” to one of “metabolic surveillance” to stay ahead of metastatic disease. This proactive infrastructure acts as an insurance policy against both patient mortality and institutional liability. Investing in these prevention steps today will safeguard the health of the community and the fiscal health of the organization for decades to come.
Carethix Key Takeaway
Our analysis is clear: Nigel’s death was not a medical mystery but a failure of institutional imagination and technological adoption. You must realize that “conservative management” of persistent pain is often a death sentence in the context of asymptomatic oncology. We believe that the integration of AI-driven breath analysis is no longer a luxury but a fundamental requirement for any B2B healthcare provider aiming for clinical excellence.
If your network continues to rely on physical exams and basic blood work for deep-tissue cancers, you are accepting a 13% survival rate as your standard of care. We demand a shift toward proactive, sensor-based diagnostics to ensure that 24 doctor visits lead to a cure, not a casket. The financial and moral cost of inaction is too high for the modern healthcare enterprise to ignore.
FAQs:
Why did 24 primary care visits still fail to detect pancreatic cancer before a terminal diagnosis?
Because repeated low-risk assumptions often override escalation logic, and every unresolved repeat visit should trigger mandatory diagnostic review instead of routine symptom recycling.
How can 67,530 projected 2026 pancreatic cancer cases be reduced through earlier detection systems?
Health systems must stop treating early screening as optional and deploy AI triage, biomarker pathways, and faster imaging access before cases reach advanced stages.
Why does pancreatic cancer survival fall from 44% localized to just 3% metastatic stage?
The brutal survival gap proves that delayed diagnosis is often the real killer, making speed-to-detection more valuable than late-stage treatment intensity.
Can 90% accurate breathomics technology solve persistent missed cancer diagnoses in primary care?
Breath-based screening shows promise, but leaders must integrate it into workflows with accountability metrics or it risks becoming another underused innovation.
How can reducing average treatment cost from $200,000 to $45,000 improve healthcare ROI?
The smartest cost-cutting strategy is not cheaper treatment but earlier diagnosis, where prevention economics outperform end-stage spending every time.

