
Carethix reveals how a £24K dementia-care investment can sustainably reduce costs, delirium risk, and hospital stays for better clinical outcomes.
Dementia‑Friendly Rooms at John Radcliffe: A High‑Impact Case Study
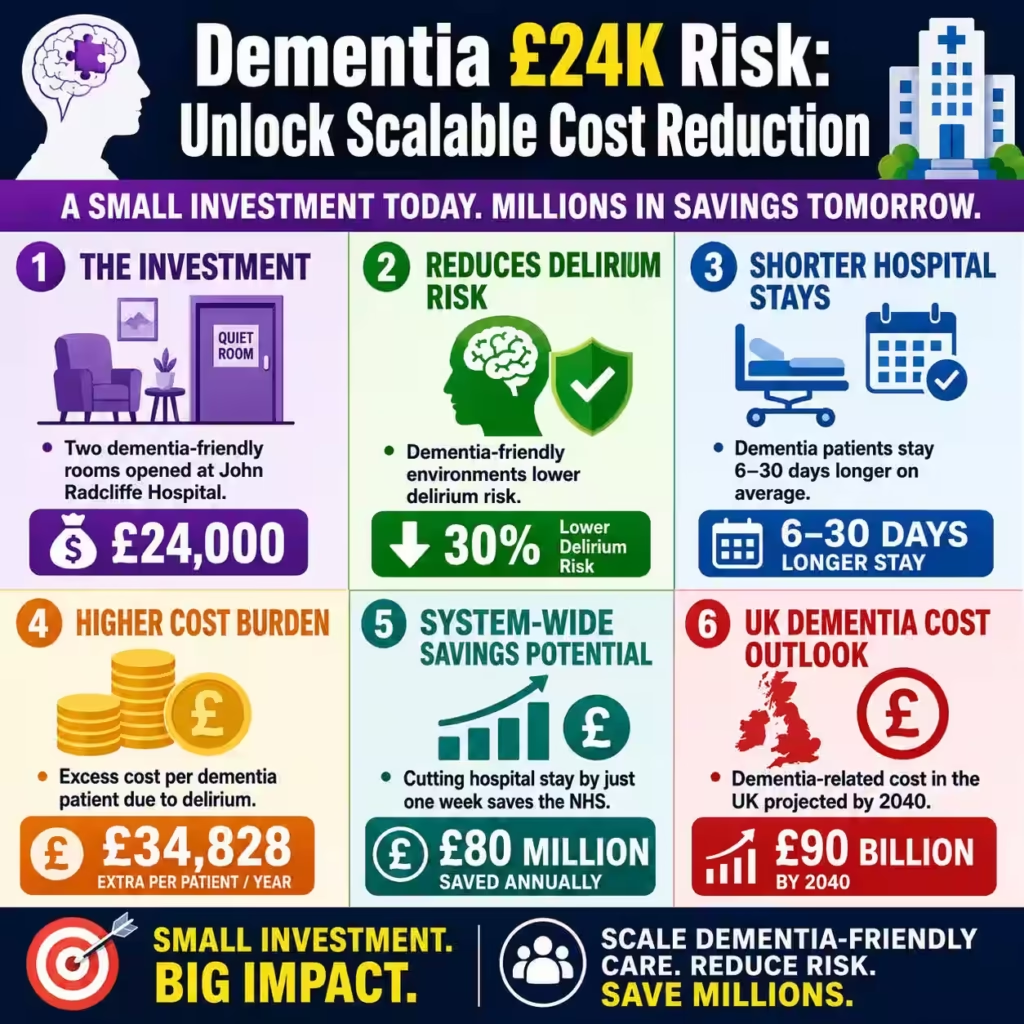
Oxford University Hospitals (OUH) has just opened two dementia‑friendly spaces at the John Radcliffe Hospital’s Complex Medical Unit, funded by Oxford Hospitals Charity with a £24,000 contribution. These spaces—the Quiet Room and the Patient Activity Room—are designed to reduce delirium risk, length of stay, and long‑term healthcare costs for older, cognitively impaired patients. For a trust that already faces pressure from a rising dementia cohort, this £24,000 investment is a targeted, asset‑light intervention with measurable upside.
Dementia patients consistently incur longer hospital stays than peers without cognitive impairment, averaging roughly 6–30 days longer in many NHS acute trusts. Studies of older inpatients show that delirium alone can drive an excess of about $34,828 in one‑year healthcare costs for patients with Alzheimer’s disease and related dementias (ADRD). When mapped to a large acute hospital such as OUH, repeating that excess cost across hundreds of dementia‑associated admissions translates to tens of millions of pounds in avoidable expenditure over a five‑year horizon.
The Quiet Room at John Radcliffe is positioned where Acute Rehab Support Workers can engage patients away from the busy ward, reducing environmental noise and stimulation. This aligns with evidence that suboptimal physical and social environments increase delirium, functional decline, and length of stay in people with dementia. By offering a low‑stimulation zone for cognitive rest, crisis management, and difficult family conversations, the unit is effectively converting a small capital outlay into a delirium‑reduction lever.
The second room, the Patient Activity Room, is equipped with large touchscreens preloaded with music, films, games, and audiobooks intended to support reminiscence and rehabilitation. Cognitive stimulation and structured physical activity have been linked to slower functional decline and better mood in dementia populations, which in turn can reduce discharge delay. For a ward whose elderly patients often have long hospital stays, this space is not just a “wellbeing add‑on” but a throughput‑oriented intervention that can shave days off the average length of stay.
Economically, the dementia‑related cost burden in the UK is projected to reach about £90 billion by 2040, with the average per‑person cost ranging from roughly £28,700 for mild dementia to £80,500 for severe dementia. One frequently cited estimate suggests that reducing hospital stay by just one week for dementia patients could save the NHS about £80 million annually. Viewed through that lens, a £24,000, dementia‑friendly room investment at a single site like John Radcliffe is a low‑cost generator of system‑level savings if replicated across multiple units and trusts.
Clinically and strategically, the John Radcliffe example flags a clear opportunity: retrofitting existing ward stock into cognition‑aware spaces is cheaper and faster than full dementia‑specific wards, yet it can materially influence delirium rates, patient safety, and downstream costs. Health systems that treat dementia‑friendly design as a capital‑led, one‑off project will miss the real value. The stronger framing is to treat these rooms as part of a scalable, outcomes‑driven operating model that links environment, staff training, and care pathways to measurable financial and clinical KPIs.
Carethix’s Critique: Where Dementia‑Friendly Rooms Are Not Enough
From a B2B healthcare consultancy perspective, the John Radcliffe dementia‑friendly rooms are a positive signal, but they do not solve the core structural and financial risks that dementia poses to hospital systems. The £24,000 spend is necessary optics, but it is not sufficient to address delirium‑driven cost escalations, workforce strain, and discharge delays that already run into millions of pounds per year.
First, the investment is asset‑specific and ward‑specific. The rooms are confined to the Complex Medical Unit at John Radcliffe, yet dementia‑affected patients are scattered across emergency departments, general medical wards, and surgical units in the same hospital. Without a trust‑wide, pathway‑centric approach, delirium risk, staff stress, and length‑of‑stay inflation simply shifts to other areas rather than being contained.
Second, the rooms are environment‑only levers. They do not by themselves mandate dementia‑specific protocols, staff training, or decision‑support tools for delirium screening and medication review. Evidence shows that delirium in ADRD patients is strongly associated with polypharmacy, dehydration, and untreated infections, none of which a painted wall or quiet room can directly control. A dementia‑friendly environment without a dementia‑aware clinical operating model is like buying low‑glare lighting for a building whose wiring is still overloaded.
Third, financial return is implied, not tracked. OUH and Oxford Hospitals Charity have not yet publicly committed to measuring changes in length of stay, delirium incidence, readmission rates, or family‑reported distress in the new rooms. Without a baseline–post baseline, the project appears to be a charitable “good‑citizen” move rather than a disciplined investment with a clear ROI. For a hospital finance director, that makes it difficult to justify replication or scale.
Fourth, the rooms do not address the upstream and downstream ecosystem. Dementia‑related costs are dominated by unpaid caregiving and social‑care expenditure, which account for roughly 50% and another significant share of the £42 billion current UK dementia cost burden. A hospital‑based environment intervention does little to reduce family‑care hours or prevent premature institutionalization. If the unit cannot reliably signpost and coordinate post‑hospital support, the financial and clinical benefits of the quiet room will be diluted.
Finally, the model is still rooted in charity‑funded capital. Relying on £24,000 from Oxford Hospitals Charity to fund dementia‑friendly design exposes a deeper governance gap: why is environmental adaptation for a high‑cost, high‑volume patient group being treated as philanthropy instead of core clinical infrastructure? In a financially constrained NHS, this framing risks making dementia‑friendly design episodic and discretionary rather than a standard of care.
Solutions: Building a System‑Level Dementia‑Care Operating Model
To move beyond the “two‑room” model, hospitals and health systems must embed dementia‑friendly design and care into a broader, financially defensible operating model. What follows is a set of actionable, B2B‑oriented solutions that can be tailored to your organisation’s size, payer mix, and risk profile.
Instead of one or two dementia‑friendly rooms, map where dementia‑affected patients are most frequently admitted—such as emergency short‑stay, general medicine, and orthopaedic units—and define a minimum dementia‑environment standard for each. That standard should include noise‑absorbing finishes, clear way‑finding, non‑glare lighting, and small activity or quiet zones that can be reused for multiple clinical purposes. Retrofitting over time is preferable to waiting for a new capital build, because evidence shows that even modest environmental changes can reduce delirium incidence and length of stay.
Environment alone cannot prevent delirium; robust clinical protocols and staff capability are required. Implement a trust‑wide delirium screening bundle using validated tools such as the 4AT or CAM‑ICU, with mandatory screening on admission and at least once per day while at risk. Pair this with a medication‑review checklist that flags high‑risk anticholinergics, benzodiazepines, and excessive opioids, which are strongly linked to delirium in older adults.
In parallel, deliver mandatory dementia‑awareness training for nurses, doctors, and support staff, focusing on communication, restraint‑minimisation, and early escalation of agitation or confusion. Frame this as a quality and safety investment, not a “soft” wellbeing initiative, because poor communication and mismanagement of behaviour are major drivers of restraint‑related incidents and complaints.
The John Radcliffe Quiet and Activity Rooms already use large touchscreen devices with music, games, and historical content. The next step is to treat these devices as part of a structured cognitive‑support toolkit, not simply entertainment. Curate content libraries that align with evidence‑based cognitive stimulation, reminiscence therapy, and simple physical‑activity prompts, and train staff to schedule short, repeat sessions rather than ad‑hoc use.
For larger systems, consider embedding dementia‑specific decision‑support rules into the electronic health record. These could flag high‑risk medications, prompt delirium screening, and recommend early involvement of occupational therapy or cognitive‑rehab specialists. Done correctly, this can reduce decision‑making variability across shifts and sites, which is a key driver of avoidable delirium and prolonged stays.
Hospitals and payers must move beyond paying only for volume and instead reward reductions in dementia‑associated complications. For trusts operating under a DRG‑like or tariff system, this could mean designing local contracts that reward reductions in length of stay, delirium incidence, and readmission rates for patients with dementia or cognitive impairment.
For private‑payer or integrated systems, consider risk‑adjusted bundles for older patients with dementia, where a portion of the episode payment is withheld unless the unit meets targets for delirium rates, restraint use, and family‑reported satisfaction. This forces the organisation to treat dementia‑friendly design and care as a financial priority, not a nice‑to‑have, and aligns clinical behaviour with long‑term cost control.
Prevention: Building Resilient, Dementia‑Resilient Care Pathways
If hospitals react only at the point of admission, they will remain in a reactive, high‑cost cycle. Prevention requires upstream detection, early intervention, and coordinated care before emergency admission occurs.
Early diagnosis and structured management of mild‑stage dementia can reduce later hospitalisation and delirium. Develop or expand primary‑care pathways that include routine cognitive screening for adults over 65, particularly those with multiple comorbidities or frailty, and fast‑track referrals to specialist memory clinics. Where feasible, use brief digital‑based cognitive assessments that can be administered in general practice and flag high‑risk patients for early intervention.
Evidence shows that avoiding hospital admission or shortening stay can significantly reduce dementia‑related costs. Invest in hospital‑at‑home or rapid‑response teams that can manage acute exacerbations in older adults with dementia in their own homes, supported by remote monitoring, telehealth visits, and nurse‑led home visits. This approach can reduce the need for complex medical admissions, lower delirium risk, and preserve functional independence.
Discharge planning for dementia patients is not an administrative task; it is a financial risk‑mitigation strategy. Introduce standardised discharge checklists for patients with dementia or cognitive impairment, covering medication reconciliation, home‑safety review, caregiver support, and scheduled follow‑up within 48–72 hours. Where possible, link these patients to community‑based re‑enablement services that provide short‑term home support, cognitive stimulation, and physical therapy to prevent readmission.
Poor communication with families is a major driver of complaints, escalation, and repeated admissions. Develop a standardised “dementia‑friendly communication framework” for ward staff, including the use of simple language, regular family updates, and formal family meetings for complex or high‑risk patients. Train staff in advanced communication techniques for difficult conversations about prognosis, capacity, and discharge options, so that families feel informed and supported rather than overwhelmed.
Carethix’s Key Takeaway
The new Dementia‑friendly rooms at John Radcliffe illustrate that a relatively small capital investment can yield meaningful improvements in delirium risk, patient experience, and staff working conditions. However, they also expose a broader truth: hospitals that treat dementia‑friendly design as a ward‑specific capital project will not materially reduce the £42 billion UK dementia‑related cost burden or the £34,828‑plus in excess costs per delirious ADRD patient.
For you as a healthcare executive or payer, the strategic imperative is clear. You must shift from viewing dementia‑friendly rooms as isolated charity‑funded upgrades to treating them as one component of a system‑level dementia‑care operating model that links environment, staff capability, clinical protocols, digital tools, and financial incentives. By doing so, you convert a £24,000 room into a scalable, ROI‑driven lever that can reduce length of stay, delirium, readmissions, and long‑term costs while also improving patient safety and family satisfaction.
FAQs:
How Can a £24,000 Dementia-Friendly Hospital Room Reduce NHS Delirium Costs by Millions?
A £24,000 dementia-friendly room investment at the John Radcliffe Hospital looks cost-effective because delirium in Alzheimer’s disease and related dementias (ADRD) patients can add roughly $34,828 in excess one-year healthcare costs per patient. The bigger issue is that most NHS trusts still treat dementia-friendly infrastructure as a charity-funded “wellbeing project” instead of a measurable cost-reduction strategy tied to KPIs like reduced length of stay and readmission rates. Without trust-wide rollout and financial ROI tracking, hospitals risk limiting a potentially multi-million-pound operational efficiency model to a symbolic two-room intervention.
Why Do Dementia Patients Stay 6–30 Days Longer in NHS Hospitals Compared to Other Patients?
Studies cited in the article show dementia patients can remain hospitalized 6–30 days longer than patients without cognitive impairment, largely due to delirium, poor environmental design, discharge delays, and fragmented care pathways. The criticism is that many acute hospitals still rely on overstimulating wards, inconsistent delirium screening, and undertrained staff despite knowing these operational failures directly inflate bed occupancy and workforce strain. Hospitals focusing only on capacity expansion instead of dementia-specific throughput optimization are effectively allowing avoidable inpatient costs to compound year after year.
Can Dementia-Friendly Hospital Design Really Save the NHS £80 Million Per Year?
The article highlights a widely cited estimate that reducing dementia patient hospital stays by just one week could save the NHS approximately £80 million annually. While this makes dementia-friendly design highly attractive from a healthcare economics perspective, the weakness is that most trusts fail to connect environmental redesign with mandatory delirium screening, medication review protocols, and digital decision-support systems. A quiet room alone cannot sustainably unlock £80 million in savings unless hospitals operationalize dementia care as a system-level performance model rather than a standalone capital upgrade.
What Are the Biggest Hidden Costs of Delirium and Dementia in UK Hospitals by 2040?
The UK dementia-related economic burden is projected to reach nearly £90 billion by 2040, with severe dementia costs averaging about £80,500 per person. The overlooked pain point is that hospitals continue to underestimate downstream costs tied to caregiver burnout, delayed discharge, avoidable readmissions, and institutionalization, which collectively create enormous financial leakage across the NHS and social-care ecosystem. Healthcare executives who ignore proactive dementia operating models today may face exponentially higher staffing, occupancy, and reimbursement pressures over the next decade.
Why Are Dementia-Friendly Hospital Rooms Not Enough to Prevent Readmissions and NHS Cost Escalation?
The article strongly argues that dementia-friendly rooms alone cannot address major delirium drivers such as polypharmacy, dehydration, untreated infections, and poor discharge coordination. The deeper operational problem is that many hospitals invest in visible infrastructure improvements without implementing trust-wide dementia protocols, 4AT/CAM-ICU screening, or risk-adjusted reimbursement incentives tied to outcomes. Unless hospitals integrate environment, staff training, digital tools, and family-centered discharge planning into one scalable dementia-care operating model, readmission rates and long-term dementia costs will continue escalating despite cosmetic improvements.

