
CT’s 3 pediatric deaths demand robust pediatric safety systems; discover strategic retail barriers and clinical solutions.
Deep Case Study: The Benadryl Challenge Crisis
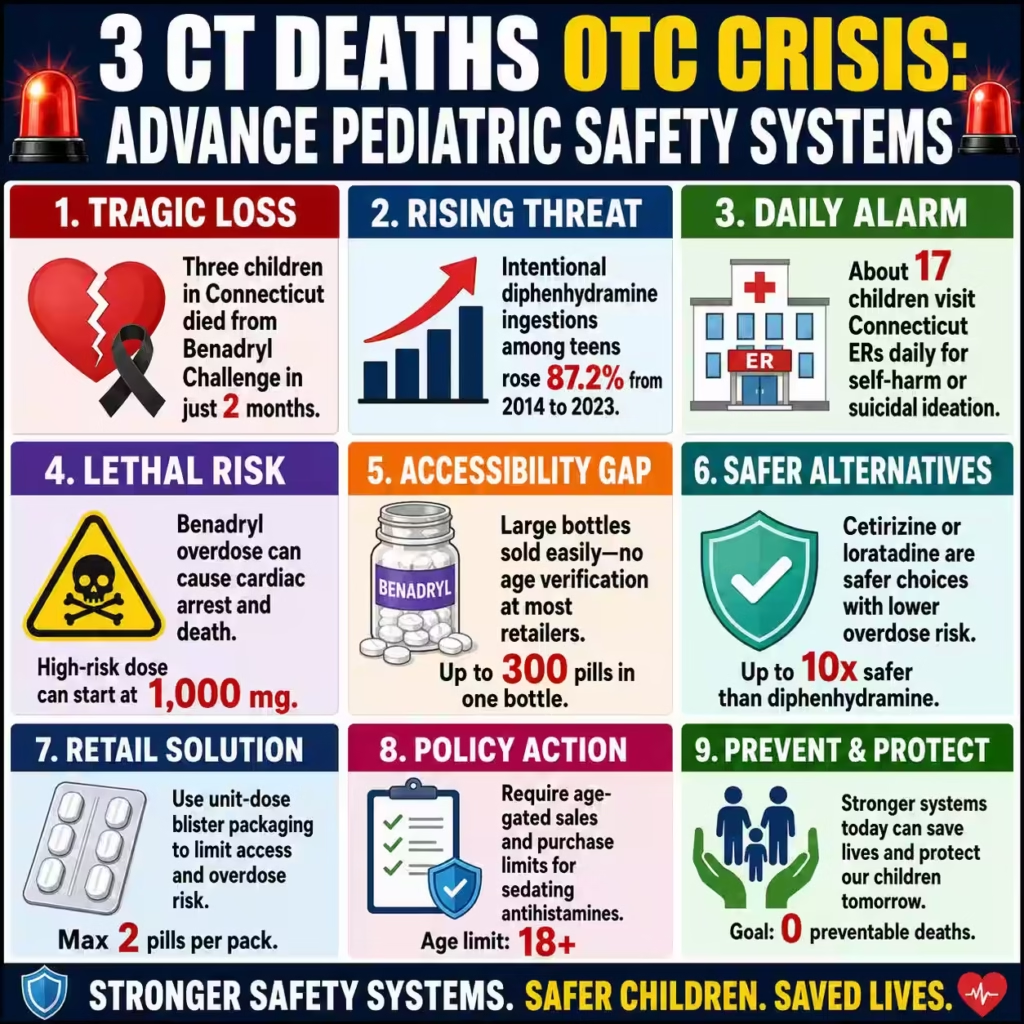
Three children in Connecticut have died within a span of just two months due to diphenhydramine overdoses linked to the viral “Benadryl Challenge.” The Connecticut Office of the Child Advocate (OCA) confirmed these fatalities, highlighting a catastrophic resurgence of a social media trend encouraging the ingestion of massive doses of this common antihistamine to induce hallucinations. This staggering loss of life underscores a critical vulnerability in our current pediatric safety architecture, where a ubiquitous household medication becomes a lethal weapon in the hands of uninformed youth.
The pain point here is the terrifying accessibility of diphenhydramine combined with the insidious reach of algorithmic peer pressure on platforms like TikTok. Jeancarllos Torres, a grieving father, poignantly asks, “What are you doing with your own kids to make them think it is okay to do Benadryl,” signaling a desperate need for parental vigilance and systemic reform. Beyond these three tragic deaths, the broader data is equally alarming; the OCA notes that approximately 17 children visit Connecticut emergency rooms daily for self-harm or suicidal ideation, creating a fertile ground for dangerous viral challenges to take hold.
Clinically, the “Benadryl Challenge” is a game of Russian roulette. The dose required to trigger the desired hallucinations is often indistinguishable from the dose that causes cardiac arrest, seizures, and death. Recent data from the National Poison Data System (NPDS) reveals an 87.2% increase in intentional diphenhydramine ingestions among adolescents from 2014 to 2023, proving this is a rising national tide rather than an isolated cluster. This statistical surge represents a compounding failure of educational, retail, and digital safeguards that demands an immediate, high-level intervention.
Yale Medicine specialists now explicitly advise against keeping Benadryl in homes with children, citing the availability of safer, non-sedating alternatives like cetirizine or loratadine which carry significantly lower overdose risks. The biological mechanism of toxicity involves anticholinergic poisoning, leading to wide-complex tachycardia and QT prolongation, which can swiftly progress to fatal arrhythmias. Each of these three Connecticut deaths was not merely an accident but a predictable outcome of a system that allows high-risk medications to be sold in bulk bottles without friction.
High-authority analysis suggests that without a radical shift in how we dispense and monitor OTC medications, these “viral” fatalities will become a permanent statistical baseline. We are witnessing a convergence of mental health crises—evidenced by the 17 daily ER visits—and unrestricted access to lethal means. The solution requires moving beyond “awareness” to implementing tangible barriers, such as mandatory blister packaging and age-gated sales for sedating antihistamines.
Carethix Critique: Systemic Gaps and Lethal Accessibility
Carethix issues a severe critique of the current regulatory and retail environment that treats diphenhydramine as a benign staple rather than a potent psychoactive compound. The death of three children in sixty days is not an anomaly; it is a direct indictment of a passive healthcare marketplace that prioritizes convenience over pediatric survival. We assert that the continued sale of diphenhydramine in large-count, loose-pill bottles constitutes gross negligence in product stewardship given the known abuse patterns.
The “Benadryl Challenge” has been a known vector of morbidity since at least 2020, yet retailers and manufacturers have failed to implement meaningful friction points to purchase. It is unacceptable that a teenager can purchase lethal quantities of diphenhydramine at a self-checkout kiosk without the same scrutiny applied to pseudoephedrine products. This regulatory gap allows the “challenge” culture to weaponize supply chain efficiencies against vulnerable populations.
Furthermore, we criticize the digital ecosystem’s sluggish response to removing content that promotes these fatal activities. While platforms claim to police harmful trends, the “Benadryl Challenge” continues to resurface with lethal consequences, indicating that current algorithmic safety nets are porous and insufficient. Carethix identifies a failure in corporate social responsibility where tech giants profit from engagement metrics driven by shock content while externalizing the mortality costs to families and healthcare systems.
The medical community also bears a portion of this burden for not aggressively phasing out diphenhydramine as a first-line recommendation for pediatric allergies. As noted by Yale experts, superior second-generation antihistamines exist that do not cross the blood-brain barrier, yet diphenhydramine remains a default “legacy” choice in many households. This clinical inertia perpetuates the presence of a dangerous toxicant in medicine cabinets, directly contributing to the “accessibility” risk factor identified in these overdoses.
Finally, the critique must address the gap in mental health infrastructure that leaves children susceptible to such reckless validation-seeking behavior. The statistic of 17 daily ER visits for self-harm in Connecticut alone suggests a youth mental health epidemic that renders “challenges” uniquely attractive as a form of dissociation or cry for help. Carethix posits that treating these deaths solely as “accidental overdoses” ignores the underlying despair and lack of supervision that drives children to ingest handfuls of pills.
Strategic Solutions: Retail Barriers and Clinical Shifts
The most immediate and effective business solution is the universal adoption of unit-dose blister packaging for all diphenhydramine products sold over the counter. Studies consistently show that blister packs significantly reduce impulsive overdoses by introducing a “friction time” that disrupts the act of mass ingestion. Retailers and manufacturers must voluntarily pivot to this packaging format immediately, or face the inevitability of legislative mandates that will force compliance at a higher cost.
Retail pharmacies must implement strict age-verification protocols for the purchase of diphenhydramine, mirroring the restrictions placed on dextromethorphan. Placing these products behind the counter or requiring ID scans at the register creates a necessary checkpoint that prevents unsupervised acquisition by minors. This “retail friction” strategy is a proven method for reducing youth access to abusable substances without banning the medication entirely.
Healthcare providers and insurance payers should financially incentivize the use of second-generation antihistamines over first-generation options. By lowering copays for cetirizine or fexofenadine and increasing the out-of-pocket cost for diphenhydramine, we can drive consumer behavior toward safer alternatives through economic leverage. Carethix recommends that major pharmacy chains proactively delist bulk diphenhydramine bottles, stocking only small-count packages to limit the “lethal load” available in a single purchase.
Digital platforms must employ advanced computer vision and natural language processing to instantly identify and suppress “challenge” content before it gains viral traction. This requires a shift from reactive moderation to proactive “safety-by-design” architectures that flag specific drug names in proximity to keywords like “trip,” “hallucinate,” or “challenge.” Financial penalties should be levied against platforms that fail to remove such content within a strict timeframe, treating digital negligence with the same severity as physical product liability.
Educational initiatives must pivot from “drug awareness” to “digital literacy” and “critical thinking” training for parents and children. We need to equip parents with the tools to audit their home inventory, treating diphenhydramine with the same caution as opioids. This includes distributing lock boxes or disposal kits with prescriptions, a low-cost high-impact investment for insurers to prevent costly ICU admissions.
Prevention Steps: Future-Proofing Pediatric Safety
Prevention begins with a “Clean Cabinet” policy, where families are educated to remove first-generation antihistamines from their homes entirely. Pediatricians should explicitly prescribe safer alternatives and advise parents to discard any remaining Benadryl, effectively eliminating the vector of overdose from the domestic environment. This cultural shift requires a concerted messaging campaign from trusted health authorities to reframe Benadryl as a specialist medication rather than a household staple.
Schools must integrate “social media survival” curriculums that specifically address the mechanics of viral trends and the physiological reality of poisoning. Rather than vague warnings, students need to understand the gruesome biological reality of anticholinergic toxicity—seizures, catheters, and cardiac arrest—to shatter the “glamorous” illusion of the high. Real-world data, such as the 5,000 ng/mL blood concentration found in fatal cases, can be used to scientifically dismantle the myths propagated by peer groups.
Legislatively, we advocate for the “Safe OTC Packaging Act,” requiring all sedating antihistamines to be sold in child-resistant, limited-quantity formats. This prevention step moves the onus of safety from the distracted parent to the regulated product, ensuring that safety is built into the physical item itself. Such legislation would also mandate distinct warning labels that explicitly state “Overdose Risk: Heart Attack and Seizure” rather than the passive “drowsiness” warnings currently used.
Parents must engage in active “digital parenting,” utilizing monitoring software to detect engagement with dangerous hashtags or content clusters. The quote from Mr. Torres, “I’m going to teach him what’s right,” encapsulates the necessity of proactive dialogue where parents explain why a trend is deadly before the algorithm suggests it. This involves regular “tech check-ins” where families discuss current online trends, normalizing skepticism toward viral challenges.
Finally, the healthcare industry must establish a real-time “toxicosurveillance” network that links ER admission data with social media analytics. By identifying spikes in specific drug-related queries or hashtags, health officials could issue “pre-spikes” warnings to schools and parents before fatalities occur. This predictive prevention model uses data to outpace the viral spread, allowing communities to lock down medications before the wave of challenges hits their local demographics.
Carethix Key Takeaway
The death of three children in Connecticut is a mandate for immediate, uncompromising structural change in how we manage over-the-counter risks. We cannot rely on parental vigilance alone to combat the algorithmic amplification of self-harm. Carethix asserts that the continued sale of bulk diphenhydramine is a liability we can no longer afford. You must act now: audit your inventory, support retail restrictions, and demand digital accountability. Safety is not an accident; it is an engineered outcome.

